Left unchecked, medicine can easily dominate all aspect of life. This hits people at all stages of training and experience in medicine, but now that I've dipped my toe into residency, I think it likely hits residents the hardest. Residency means being both a learner and an employed junior physician, which has the unfortunate consequence of piling on both the open-ended responsibilities of a medical student to learn as much as possible, along with many (though not all) of the day-to-day responsibilities of an independent physician. Add on a situation of minimal control over one's own schedule and the need to continue to fight for a job on graduation, whether a fellowship or full employment, and medicine can easily take up every minute of the day, and every thought running through the brain.
For a small number of exceedingly passionate residents, this is exactly what they signed up for. Most residents, however, have parts of their life outside of medicine they would like to maintain or even prioritize, and that can become difficult in the metaphorical tempest of residency. Particularly when ambitions come into play, where a desired career path cannot be secured by simply showing up and performing well, medicine can push out those other, valued parts of life.
I'm finding myself falling into that trap early on in residency. I'm incredibly fortunate to be in a program with lower overall hours than many, and call schedules which are generally quite favourable. Yet this still means weeks far longer than a typical work week and the added time has largely gone towards maintaining a real sleep schedule and keeping up a rather bare-bones home life. My spare time now is still largely focused around medicine, either doing things for my career or, out of anxiety of having to do them all the time, unproductively procrastinating those activities.
As I was fairly ambitious in medical school, I've essentially been running on this medicine-focused treadmill for about 3 years straight now. I've learned this doesn't work well for my health, well-being, or even my achievement levels. I was able to scale-down my commitments later into my third year of medical school and into my fourth year. My choice to go into Family Medicine was influenced by this realization, a choice I'm quite happy with thus far if only for the sake of my own health.
Yet I'm still struggling with balancing my ambitions within medicine with my ambitions outside of my career. I want to do more as a physician, as I see so many opportunities to do a better job for patients. However, I've learned from experience that you can give everything you have to the medical system and end up causing more harm - especially to yourself and your loved ones - than you see in benefits for patients.
Prioritizing medicine above the rest of life didn't work and, in retrospect, many more senior physicians told me as much. So, I've tried to play a balancing act in the past year and a half, weighing any benefits to being more active in medicine with drawbacks to life outside of medicine. Again, for my health this has been a positive change, yet it comes with one major drawback - my life is still dominated by my medical career. Even if I choose not to pursue a new opportunity within residency, or put in an additional hour in a clinical setting, or do an extra bit of studying, I'm still making that decision with medicine as the focus. Unfortunately, this is leading to a fair bit of resentment towards my own medical career, without a countervailing positive in my non-medical life.
Therefore, I'm going to try to change tacks once again. Beyond trying to maintain a balancing act, I'm going to see how things work when life comes first. Before lifting an extra finger for the sake of a medical career that seems rather indifferent to my efforts, I'm going to try to make sure I have time for the non-medical things in life I care about. Getting a real amount of exercise. Spending quality time with my spouse. Watching the hockey game. Reading the newspaper. And if I'm really lucky, pursuing some hobbies I've had on the back-burner for years. Only then will I do the non-essential work in my medical career. My hope is that I can attack those activities in medicine with the vigor they deserve and which, over the course of the past 3 years, has waned from exhaustion and over-exposure.
Part of that is this, my Medical Blarg. This blog started as my way of actively de-stressing about being a medical student. As it unexpectedly gained viewership, it felt like the one activity in medicine that was leading to something productive. The encouragement to keep going from posters was immensely appreciated. Yet, it's hard for me to deny that as a result of its viewership, this blog has, in a way, also become a part of my medical career. There reached a time when posting felt more like an obligation that the enjoyable exercise it started out as. As a result, I've pulled back a bit on my posting frequency. My hope is that doing so allows me to continue to blog, but with a bit more enthusiasm and genuineness that I have been able to in the past few months.
Sunday, 27 August 2017
Thursday, 10 August 2017
Residency, Block One
Well, I just finished up my first block of residency. Starting on my home rotation of Family Medicine, I got a chance to dive right into what I hope to be doing for the rest of my career. It's been a very busy transition (hence the complete lack of posting), but in a mostly good way. Here are my first impressions.
1) Increased Responsibility
This hit harder than I expected, and faster. I see my own patients. I review most of them with my preceptor, but not all of them. My preceptor sees my patients usually only when I ask them to. I can write my own prescriptions now - I even have a stamp with my name on it for those! It's a wonderful freedom in many respects, as I don't have to couch every single encounter based on what I think my preceptor wants. Instead, I can give my own impression and hedge only when I'm uncertain about the best answer.
Yet, that means when I mess up, it's all on me. And I've definitely messed up. No big screw-ups - life-or-limb cases are fortunately not that common in Family Medicine and I know enough to at least confirm my thoughts with my preceptor in these cases - but certainly less-than-optimal actions that could have been handled better. I recognize that's part of the learning process and that in my first rotation is very much expected, but it still hits a bit harder now than it did in medical school. As a student, if a patient's treatment was sub-optimal because of my mistake, outside of a clearly negligent decision, much of the fault would lie with the educational system that either failed to properly train or supervise my actions. Now those factors still matter, as I'm still a trainee, but as an employee, I share far more in that responsibility.
2) Rush, Rush, Rush
When I started my rotation, I got a slow introduction. Lots of time for patient appointments. Arguably too much time. I was getting bored going into my second week, and started asking to see more patients. Then I got ramped up to a full schedule in my third week. It. Was. Crazy. I managed to keep up with my schedule, yet only at the expense of my note-writing. On the busier days, I was at the clinic hours afterwards finishing my notes and completing other paperwork.
Nevertheless, I mostly kept my head above water and I'm fairly proud of that fact. At the end of my block, I was handling a workload roughly what I can expect as an early PGY-2 and while I wasn't nearly as consistent or efficient as the PGY-2's in the office (who were nothing short of amazing), I at least did the job. As I gain some more experience and familiarity, I'm hoping the late nights of note-writing well decrease.
That said, even my current "full schedule" pace is about half what it will be in full practice. Even with the advantages of a shorter lunch (currently I get over an hour, which I don't really need), lighter note requirements (my notes are detailed now, especially compared to the 2-3 lines most of my preceptors write), an extra exam room (I get a single room now), and no delays caused by checking with a preceptor, I'm nowhere near being able to operate at full speed. Yet, I've got 25 more blocks, including many family medicine blocks, to get up to that pace, so there's still plenty of time.
3) Home Call is Not Like In-House Call
One of the interesting quirks to my residency program is that we do a full home call on our Family Medicine blocks. It's not particularly frequent (about one weeknight every 2 weeks and one weekend every 2 months) and in many Family Medicine centres, it wouldn't be too busy. Except at my centre. Our weekend call is Friday night through until Monday morning. I got at least two dozen calls during that time, some of which were simple and straight-forward, others which took a fair bit of time to sort out. Ended up having to do a fair bit of driving, either to see patients in clinic over the weekend or to visit patients in the nursing home we cover.
The main advantage of home call is that you can still do life-stuff when you're not actively working. That's pretty great, since you can get a lot done if you don't get called often. It's way better than in-house call in that respect, where you're basically working a 24-hr shift that may involve some long breaks if you're lucky, but which doesn't allow you to do anything outside of the hospital. Yet, since my home call was over 60 hours long and was reasonably busy - during the day, I rarely got more than an hour off - I didn't get much opportunity to get anything done and developed some rather intense pager anxiety. It's surprisingly hard to "switch off" on the third day of being page-able at any time!
4) Conclusions
Overall, I'm enjoying residency more than I did medical school. There's a bit more independence and some clear ways to progress forward over time. Getting paid rather than paying insane amounts of tuition is a significant benefit, as finances are now slowly moving in the right direction. Month-long blocks rather than two week rotations provides a bit of stability, and the ability to take vacations provides some much-needed flexibility, though the schedule remains fairly hectic.
Life still isn't yet where I'd like it to be - I spend too much time at work or on work and don't have enough consistency or control over my own schedule to prioritize other aspects of living. I'll be glad to finally finish up in two years' time and to experience the supposed wonder of full, independent practice. Nevertheless, residency feels closer to my ultimate lifestyle goals than medical school did and what sacrifices are necessary feel more like they're in the service of meaningful progress than they did as a medical student.
1) Increased Responsibility
This hit harder than I expected, and faster. I see my own patients. I review most of them with my preceptor, but not all of them. My preceptor sees my patients usually only when I ask them to. I can write my own prescriptions now - I even have a stamp with my name on it for those! It's a wonderful freedom in many respects, as I don't have to couch every single encounter based on what I think my preceptor wants. Instead, I can give my own impression and hedge only when I'm uncertain about the best answer.
Yet, that means when I mess up, it's all on me. And I've definitely messed up. No big screw-ups - life-or-limb cases are fortunately not that common in Family Medicine and I know enough to at least confirm my thoughts with my preceptor in these cases - but certainly less-than-optimal actions that could have been handled better. I recognize that's part of the learning process and that in my first rotation is very much expected, but it still hits a bit harder now than it did in medical school. As a student, if a patient's treatment was sub-optimal because of my mistake, outside of a clearly negligent decision, much of the fault would lie with the educational system that either failed to properly train or supervise my actions. Now those factors still matter, as I'm still a trainee, but as an employee, I share far more in that responsibility.
2) Rush, Rush, Rush
When I started my rotation, I got a slow introduction. Lots of time for patient appointments. Arguably too much time. I was getting bored going into my second week, and started asking to see more patients. Then I got ramped up to a full schedule in my third week. It. Was. Crazy. I managed to keep up with my schedule, yet only at the expense of my note-writing. On the busier days, I was at the clinic hours afterwards finishing my notes and completing other paperwork.
Nevertheless, I mostly kept my head above water and I'm fairly proud of that fact. At the end of my block, I was handling a workload roughly what I can expect as an early PGY-2 and while I wasn't nearly as consistent or efficient as the PGY-2's in the office (who were nothing short of amazing), I at least did the job. As I gain some more experience and familiarity, I'm hoping the late nights of note-writing well decrease.
That said, even my current "full schedule" pace is about half what it will be in full practice. Even with the advantages of a shorter lunch (currently I get over an hour, which I don't really need), lighter note requirements (my notes are detailed now, especially compared to the 2-3 lines most of my preceptors write), an extra exam room (I get a single room now), and no delays caused by checking with a preceptor, I'm nowhere near being able to operate at full speed. Yet, I've got 25 more blocks, including many family medicine blocks, to get up to that pace, so there's still plenty of time.
3) Home Call is Not Like In-House Call
One of the interesting quirks to my residency program is that we do a full home call on our Family Medicine blocks. It's not particularly frequent (about one weeknight every 2 weeks and one weekend every 2 months) and in many Family Medicine centres, it wouldn't be too busy. Except at my centre. Our weekend call is Friday night through until Monday morning. I got at least two dozen calls during that time, some of which were simple and straight-forward, others which took a fair bit of time to sort out. Ended up having to do a fair bit of driving, either to see patients in clinic over the weekend or to visit patients in the nursing home we cover.
The main advantage of home call is that you can still do life-stuff when you're not actively working. That's pretty great, since you can get a lot done if you don't get called often. It's way better than in-house call in that respect, where you're basically working a 24-hr shift that may involve some long breaks if you're lucky, but which doesn't allow you to do anything outside of the hospital. Yet, since my home call was over 60 hours long and was reasonably busy - during the day, I rarely got more than an hour off - I didn't get much opportunity to get anything done and developed some rather intense pager anxiety. It's surprisingly hard to "switch off" on the third day of being page-able at any time!
4) Conclusions
Overall, I'm enjoying residency more than I did medical school. There's a bit more independence and some clear ways to progress forward over time. Getting paid rather than paying insane amounts of tuition is a significant benefit, as finances are now slowly moving in the right direction. Month-long blocks rather than two week rotations provides a bit of stability, and the ability to take vacations provides some much-needed flexibility, though the schedule remains fairly hectic.
Life still isn't yet where I'd like it to be - I spend too much time at work or on work and don't have enough consistency or control over my own schedule to prioritize other aspects of living. I'll be glad to finally finish up in two years' time and to experience the supposed wonder of full, independent practice. Nevertheless, residency feels closer to my ultimate lifestyle goals than medical school did and what sacrifices are necessary feel more like they're in the service of meaningful progress than they did as a medical student.
Tuesday, 27 June 2017
Practicing Medicine with an MD Only
The tragic story of Dr Robert Chu is making the rounds on social media after a profile in the Toronto Star and an accompanying piece about the troublesome nature of the CaRMS match that did not provide him a residency position despite two application cycles. His is a horrific end that highlights the high-stress, low-support nature of medicine in general, but particularly for those who hit speed bumps on their path to becoming a physician.
Many words have been written or spoken about how to remedy situations like this and prevent outcomes like Dr Chu's. These are important topics to discuss which for far too long have been left unaddressed in actions if not in words. I wish these conversations were happening independent of this story, however, as there is so much unknown about Dr Chu's situation that it prevents his particular circumstances from being meaningfully addressed and throws his death into the middle of a discussion that is much, much bigger than his individual story, significant as it is.
There are numerous responses being discussed, but I wanted to focus on one of them. Namely, that having an MD, even without any residency training, should permit someone to work in healthcare in some capacity. Indeed, an MD is rather unique among degrees in that, on its own, means very little. Even in fields where additional training is often necessary, the introductory degree still holds value and can be used to pursue various career paths. The MD is, in effect, a useless degree.
This idea has been circulating among American physicians for some time, even if it hasn't gained much traction in Canada, in no small part due to the increasing presence of Physician Assistants (PAs) and Nurse Practitioners (NPs) in the US. Particularly when it comes to PAs, American physicians see people who have spent less time training than a freshly-graduated MD who cannot work independently, but are able to essentially practice medicine under a qualified physician. This begs the question as to why MDs who were unable to match couldn't do the same. It may not even be overly difficult to set up such a system, as PAs don't have much legal authority themselves, but work under the framework of delegation legislated for physicians. The legal and regulatory framework is largely in place already to allow supervised MD practice without residency, under the direction of a fully-trained physician.
Yet, as things currently stand, I would not being in favour of letting MDs practice in a manner similar to PAs. While MD training is longer, and thus both deeper and broader than that for PAs, it's not particularly functional. MDs are trained more to know rather than to do. PAs are trained to work as they were intended as soon as they graduate. A fresh PA is essentially an extra arm to a physician, allowing them to do more using their already-established knowledge. A fresh MD is more like an extra brain, which isn't particularly helpful to a fully-trained physician who already has that knowledge in spades.
Updating training within MD programs to emphasize practical skills above knowledge could solve this problem and set physicians up to have some sort of back-up option if they fail to land a residency. I'd far prefer a set-up like this with continual supervised practice as opposed to something like the old rotating internship leading to the ability to work as a GP after only a year of post-graduate training. This would require a fairly massive shift in medical education from the current approach, all at a time when getting even small adjustments is an uphill battle. Still, I believe that making medical student education more practical and focused on what we do rather than what we know is worthwhile on its own merits, independent of its implications for the job market.
So, it's an option I think should be considered in these sorts of discussions. It's not the simplest solution (that would be simply making moves to improve the student-to-residency spot ratio) and it's not without its flaws. However, I think it could fit into a broader approach to improving medical education that moves the profession forward.
Many words have been written or spoken about how to remedy situations like this and prevent outcomes like Dr Chu's. These are important topics to discuss which for far too long have been left unaddressed in actions if not in words. I wish these conversations were happening independent of this story, however, as there is so much unknown about Dr Chu's situation that it prevents his particular circumstances from being meaningfully addressed and throws his death into the middle of a discussion that is much, much bigger than his individual story, significant as it is.
There are numerous responses being discussed, but I wanted to focus on one of them. Namely, that having an MD, even without any residency training, should permit someone to work in healthcare in some capacity. Indeed, an MD is rather unique among degrees in that, on its own, means very little. Even in fields where additional training is often necessary, the introductory degree still holds value and can be used to pursue various career paths. The MD is, in effect, a useless degree.
This idea has been circulating among American physicians for some time, even if it hasn't gained much traction in Canada, in no small part due to the increasing presence of Physician Assistants (PAs) and Nurse Practitioners (NPs) in the US. Particularly when it comes to PAs, American physicians see people who have spent less time training than a freshly-graduated MD who cannot work independently, but are able to essentially practice medicine under a qualified physician. This begs the question as to why MDs who were unable to match couldn't do the same. It may not even be overly difficult to set up such a system, as PAs don't have much legal authority themselves, but work under the framework of delegation legislated for physicians. The legal and regulatory framework is largely in place already to allow supervised MD practice without residency, under the direction of a fully-trained physician.
Yet, as things currently stand, I would not being in favour of letting MDs practice in a manner similar to PAs. While MD training is longer, and thus both deeper and broader than that for PAs, it's not particularly functional. MDs are trained more to know rather than to do. PAs are trained to work as they were intended as soon as they graduate. A fresh PA is essentially an extra arm to a physician, allowing them to do more using their already-established knowledge. A fresh MD is more like an extra brain, which isn't particularly helpful to a fully-trained physician who already has that knowledge in spades.
Updating training within MD programs to emphasize practical skills above knowledge could solve this problem and set physicians up to have some sort of back-up option if they fail to land a residency. I'd far prefer a set-up like this with continual supervised practice as opposed to something like the old rotating internship leading to the ability to work as a GP after only a year of post-graduate training. This would require a fairly massive shift in medical education from the current approach, all at a time when getting even small adjustments is an uphill battle. Still, I believe that making medical student education more practical and focused on what we do rather than what we know is worthwhile on its own merits, independent of its implications for the job market.
So, it's an option I think should be considered in these sorts of discussions. It's not the simplest solution (that would be simply making moves to improve the student-to-residency spot ratio) and it's not without its flaws. However, I think it could fit into a broader approach to improving medical education that moves the profession forward.
Tuesday, 13 June 2017
Ontario Binding Arbitration Framework
The OMA and the Ontario Government, against all odds, have come to an agreement. A preliminary one. On how to approach a real agreement. This isn't a physician services agreement, which is what would be needed to provide for a real update of physician funding schemes, but it's a start. Effectively, this sets the stage for negotiations and provides a framework to come to an agreement through a binding arbitration system.
In rejecting the previous tentative physician services agreement, I had two main concerns. First, that the presence of a defined, limited physician services budget with clawbacks on physicians as a whole put too much responsibility on individuals physicians for results beyond their power to affect. Worse, it set up an economic situation that would further encourage physicians to bill and practice in ways that advantaged them at the expense of patients, taxpayers, and their own colleagues. Second, it did not provide any protections for physicians against decision-making of the Ontario government, which is vitally important as physicians have minimal protections from current labour laws and no practical ability to strike in the event of a protracted labour dispute.
This agreement, the Binding Arbitration Framework, effectively has the Ontario government yielding the second point entirely. If this framework is agreed to, we have binding arbitration now and, by the looks of it, moving forward to future negotiations. It appears to be a reasonable solid arrangement, without much in the way of loopholes. The worst criticism I've read is that the government maintains policy-making rights, including which services should be funded which... of course they do. I doubt we could remove that in an agreement regardless of how it was written, thanks to the current Canadian constitution and the Canada Health Act. This was always going to be a loophole, but it'd be extremely inconvenient - politically and legally - for the government to take advantage of this under the proposed framework.
More interestingly, the framework touches on the first point of concern I had as well. It doesn't remove a set physician services budget, which I still find worrisome, but neuters its effectiveness considerably. First, it makes the budget subject to binding arbitration. Second, it explicitly dictates factors that an arbiter should consider, most importantly demographic changes. It does include consideration for the economic situation in Ontario, which is troublesome from an administration that has used any hint of economic weakness to justify public service cuts, but could end up being beneficial as well, as economic strength should work in our favour. Third, and most importantly, breaches in the cap on the physician services budget do not automatically result in punitive action against physicians. Rather, breaches will be subject to arbitration, where it can be determined to what extent, if any, physicians are responsible. Additionally, any punitive actions are subject to negotiation and arbitration, meaning more targeted cuts are possible, in contrast to the current approach of across-the-board cuts. I'd rather see the physician services budget cap removed entirely, but this is a reasonably well-tailored way to maintain its existence while blunting the more objectionable aspects to such a cap.
Some other objections to this agreement have been raised, however. First is that it generally precludes negotiation on the unilateral changes enacted since 2014. Yet, I haven't seen any indication this would be on the table - even the most favourable labour decisions wouldn't include significant back-payments and the OMA has little bargaining power for this time (due in no small part to its own actions). There's what's ideal and there's what's realistic; getting any meaningful compensation for the last 3 years during (failed) negotiations seems like a pipe dream more than anything. Second, the agreement limits ability to engage in strikes or job actions that directly affect patient care... which we couldn't (and shouldn't) do anyway. Job actions that negatively affect patient care in a meaningful way, including strikes, contravene recommended ethical guidelines, including those listed by the CPSO, our regulatory body. Furthermore, physician strikes don't work. The history of them in Canada is full of physicians losing badly. While recognizing a significant desire among Ontario physicians to engage in job actions, if this agreement prevents that, it'll only be saving us from ourselves.
I think I've painted a fairly clear picture of where I stand on this framework. It's not perfect, far from it. Yet, it gives Ontario physicians clear, long-term wins that looked unlikely even a few months ago. The compromises for those wins, while not insignificant, are tolerable. Critically, these benefits come before money is even on the table - I honestly figured that to gain some of these concessions moving forward, physicians would have to endure more financial pain in the short-term. To have them arranged in advance of the negotiations for the current physician services agreement would be a welcome surprise. I rejected the previous tPSA, loudly and proudly. I just voted in favour of this framework.
In rejecting the previous tentative physician services agreement, I had two main concerns. First, that the presence of a defined, limited physician services budget with clawbacks on physicians as a whole put too much responsibility on individuals physicians for results beyond their power to affect. Worse, it set up an economic situation that would further encourage physicians to bill and practice in ways that advantaged them at the expense of patients, taxpayers, and their own colleagues. Second, it did not provide any protections for physicians against decision-making of the Ontario government, which is vitally important as physicians have minimal protections from current labour laws and no practical ability to strike in the event of a protracted labour dispute.
This agreement, the Binding Arbitration Framework, effectively has the Ontario government yielding the second point entirely. If this framework is agreed to, we have binding arbitration now and, by the looks of it, moving forward to future negotiations. It appears to be a reasonable solid arrangement, without much in the way of loopholes. The worst criticism I've read is that the government maintains policy-making rights, including which services should be funded which... of course they do. I doubt we could remove that in an agreement regardless of how it was written, thanks to the current Canadian constitution and the Canada Health Act. This was always going to be a loophole, but it'd be extremely inconvenient - politically and legally - for the government to take advantage of this under the proposed framework.
More interestingly, the framework touches on the first point of concern I had as well. It doesn't remove a set physician services budget, which I still find worrisome, but neuters its effectiveness considerably. First, it makes the budget subject to binding arbitration. Second, it explicitly dictates factors that an arbiter should consider, most importantly demographic changes. It does include consideration for the economic situation in Ontario, which is troublesome from an administration that has used any hint of economic weakness to justify public service cuts, but could end up being beneficial as well, as economic strength should work in our favour. Third, and most importantly, breaches in the cap on the physician services budget do not automatically result in punitive action against physicians. Rather, breaches will be subject to arbitration, where it can be determined to what extent, if any, physicians are responsible. Additionally, any punitive actions are subject to negotiation and arbitration, meaning more targeted cuts are possible, in contrast to the current approach of across-the-board cuts. I'd rather see the physician services budget cap removed entirely, but this is a reasonably well-tailored way to maintain its existence while blunting the more objectionable aspects to such a cap.
Some other objections to this agreement have been raised, however. First is that it generally precludes negotiation on the unilateral changes enacted since 2014. Yet, I haven't seen any indication this would be on the table - even the most favourable labour decisions wouldn't include significant back-payments and the OMA has little bargaining power for this time (due in no small part to its own actions). There's what's ideal and there's what's realistic; getting any meaningful compensation for the last 3 years during (failed) negotiations seems like a pipe dream more than anything. Second, the agreement limits ability to engage in strikes or job actions that directly affect patient care... which we couldn't (and shouldn't) do anyway. Job actions that negatively affect patient care in a meaningful way, including strikes, contravene recommended ethical guidelines, including those listed by the CPSO, our regulatory body. Furthermore, physician strikes don't work. The history of them in Canada is full of physicians losing badly. While recognizing a significant desire among Ontario physicians to engage in job actions, if this agreement prevents that, it'll only be saving us from ourselves.
I think I've painted a fairly clear picture of where I stand on this framework. It's not perfect, far from it. Yet, it gives Ontario physicians clear, long-term wins that looked unlikely even a few months ago. The compromises for those wins, while not insignificant, are tolerable. Critically, these benefits come before money is even on the table - I honestly figured that to gain some of these concessions moving forward, physicians would have to endure more financial pain in the short-term. To have them arranged in advance of the negotiations for the current physician services agreement would be a welcome surprise. I rejected the previous tPSA, loudly and proudly. I just voted in favour of this framework.
Saturday, 3 June 2017
The Worst Part of Medical Training
While working on another post, I found the following paragraphs saved as a draft post. I'm not sure if I'm the author of these words and suspect that I'm not, yet can't find who wrote them originally. I have a feeling this was a forum post that ended up getting deleted, that I copied because I felt the words were worth saving.
I present them here as I found them in my draft folder - if the original author comes across this and wants them removed, I will happily do so. However, I think these paragraphs provide an important context to medical training which should be shared.
I present them here as I found them in my draft folder - if the original author comes across this and wants them removed, I will happily do so. However, I think these paragraphs provide an important context to medical training which should be shared.
"I have to highlight this for those considering or early in their medical training, because it's a part of medical training no one appreciates until they're in it.
As a trainee, there will be times where a patient's treatment is below what you consider acceptable. The worst is when there's a preceptor acting completely inappropriately. All you can do is sit back and watch the carnage unfold. If you're lucky, you'll be able to debrief the patient and provide some more appropriate guidance, as well as a bit of simple human empathy.
More often you're simply a cog in a system failing patients that, because you're new to that system, you don't understand and are ill-equipped to navigate. You act the way you think you're supposed to act, even the way others expect you to act, and it causes harm to patients in one way or another. Everyone goes along like it's normal or, worse, thanks you for your part in it. Yet, you have to continue with your role as that cog, because as a trainee, you have no alternative short of quitting. As you gain experience, becoming more knowledgeable about medicine as well as the healthcare system you're now a part of, you start to see opportunities to work around the system to avoid causing harm, to lessen it, or at least to warn patients of what's coming so they aren't blindsided.
This is the worst part of medical training - not the long hours, not the pressure to perform, not the vast amount of knowledge you need to acquire, not even the (fortunately uncommon in my experience) instances where you're personally treated poorly by preceptors - but the time where you're made to be complicit in bad care or outright mistreatment of patients. You don't have the power to change it, and so ultimately you aren't responsible for it, but it sure doesn't feel like it at the time."
I am now about a month away from starting my residency. This is definitely the part of my medical education thus far that I hated the most. It's the part of my upcoming residency I most fear. This is the dark side of medicine, the part that doesn't just challenge your ability, but compels you towards the corruption of your own ideals - ideals which the profession purports to share and uphold, yet frequently betrays.
Saturday, 27 May 2017
Working Hard and Being Successful
I've been reading about and discussing socioeconomic barriers to success lately, particularly as it relates to medicine. I also had an opportunity to be a very small part of an outreach program aimed at increasing interest in medicine in youth from disadvantaged backgrounds. One aspect to socioeconomic disadvantage I've found myself increasingly reflecting on is how multifaceted and variable this disadvantage can be. Thinking back, I've found most conversations on socioeconomic disadvantage tend to treat it as more uniform or monolithic than it is, and I've fallen into that trap of thinking too often as well. Perhaps others have come to this realization and I'm just behind in the thought-process, but I'd like to take a post to spell things out a little bit for my own sake.
To be perhaps a bit over-simplistic, I see a few distinct ways in which low socioeconomic status can manifest itself into real barriers to achievement. First is a simple lack of resources, which tends to be the focus of many interventions to assist those from lower socioeconomic backgrounds. It's undoubtedly a major problem - if some people can pay for things that others can't, and those things either directly or indirectly lead to personal achievement, then wealthier individuals will naturally benefit over their less-wealthy counterparts. In medicine these lead to some obvious and not-so-obvious barriers. To get into medicine, a student needs to pay for their undergraduate education, the MCAT, application fees, travel to interviews, and interview attire. These are not small expenses, especially when added together. However, that's just the bare minimum. Things money can buy that aren't necessary, but very helpful for getting into medical school include taking extra courses or second degrees (or even doing medical school outside of Canada), taking various prep courses or receiving extra tutoring, spending more time on unpaid extra-curriculars, or even paying for certain extra-curriculars.
Yet these examples hit only the "economic" portion of socioeconomic status. To get into medical school, there is also a significant social component that I don't believe gets recognized as often as it perhaps should. One is the development of baseline skills that many people take for granted. To use an extreme example, if a person was never taught how to read, they won't get into medical school, no matter how intelligent, responsible, and personable they might be. They can, of course, learn how to read and then start to move towards medicine, but it's a difficult skill to learn in adulthood and fundamental to all the steps that come after it. It's also a skill that typically requires significant support from others. We're lucky that in Canada most people get that support as children, but there are other skills which are not provided as reliably by our primary or secondary education system. One that springs to mind is professional communication skills, which are sorely lacking in formal education. The ability to write a concise, polite, effective e-mail has enormous benefits in securing various opportunities on a path to medicine, yet this may not be a skill some individuals even see from their elders or peers if they grow up in a setting without business people or other professionals in their lives. It's a skill that can be developed, but this takes time, support, and a certain degree of trial-and-error that more initiated individuals will not have to go through.
Likewise, access to opportunities is far from equitable across individuals of different social status. One example that comes to mind is students who happen to have physicians as parents. These parents hear about or inquire about opportunities with their colleagues and provide a point of introduction for their children. These students must still show they are worthy of those opportunities and perform well once they secure them to advance further, but that first step is often a critical one. More importantly, opportunities create a snowball effect, where prior experience justifies acceptance to future opportunities, up to and including medical school. That is, individuals with higher social status and more connections can turn into seemingly more capable applicants - and may actually be more capable applicants - due to these connections, completely unrelated to ability or effort.
I'd like to emphasize that higher socioeconomic status does not remove the need for hard work or eliminate the role of a certain degree of natural ability in the process. Medicine, like many fields, is full of well-off individuals, but these people have nevertheless put in significant effort to get to where they are. However, what my recent experiences have reminded me of is that while hard work is necessary for success, it is not sufficient on its own, hence the title of this piece. Without trying to set up too much of a strawman, I think some well-off individuals give too much credit to their own hard work in achieving success, because they started to see success when they started putting in the effort. Yet these individuals started seeing success after they started to work harder towards success because everything else was already set up for them. I've met plenty of people who haven't had the same experience, where hard work perhaps improved their situations, but that improvement was limited due to factors beyond their control.
Bringing this back to the original point about the multifaceted nature of socioeconomic disadvantage for a minute, I now worry more that many interventions to improve such disadvantage are perhaps too simplistic to be effective. We can throw money at a problem but it can end up being a waste if the more social aspects to disadvantage are left unaddressed. On the flip side, we could try to improve these social elements, yet see minimal results if resources are still lacking. However, on a more positive note, this also means that there are many different ways we can make marginal improvements in peoples' lives. If we don't have money to help, we can volunteer time to teach new skills, or provide connections that might otherwise being lacking. If we're busy and running off our feet, financial supports can nevertheless be valuable. When people move up the socioeconomic ladder, patchwork systems of support like this can be an important reason why, allowing them to fully utilize their own natural talents and work ethic.
From a personal perspective, as I move forward within my own career in medicine, I'm hoping there will be more opportunities to level the playing field a little bit - and I hope I'll have the good sense to recognize when those opportunities arise.
To be perhaps a bit over-simplistic, I see a few distinct ways in which low socioeconomic status can manifest itself into real barriers to achievement. First is a simple lack of resources, which tends to be the focus of many interventions to assist those from lower socioeconomic backgrounds. It's undoubtedly a major problem - if some people can pay for things that others can't, and those things either directly or indirectly lead to personal achievement, then wealthier individuals will naturally benefit over their less-wealthy counterparts. In medicine these lead to some obvious and not-so-obvious barriers. To get into medicine, a student needs to pay for their undergraduate education, the MCAT, application fees, travel to interviews, and interview attire. These are not small expenses, especially when added together. However, that's just the bare minimum. Things money can buy that aren't necessary, but very helpful for getting into medical school include taking extra courses or second degrees (or even doing medical school outside of Canada), taking various prep courses or receiving extra tutoring, spending more time on unpaid extra-curriculars, or even paying for certain extra-curriculars.
Yet these examples hit only the "economic" portion of socioeconomic status. To get into medical school, there is also a significant social component that I don't believe gets recognized as often as it perhaps should. One is the development of baseline skills that many people take for granted. To use an extreme example, if a person was never taught how to read, they won't get into medical school, no matter how intelligent, responsible, and personable they might be. They can, of course, learn how to read and then start to move towards medicine, but it's a difficult skill to learn in adulthood and fundamental to all the steps that come after it. It's also a skill that typically requires significant support from others. We're lucky that in Canada most people get that support as children, but there are other skills which are not provided as reliably by our primary or secondary education system. One that springs to mind is professional communication skills, which are sorely lacking in formal education. The ability to write a concise, polite, effective e-mail has enormous benefits in securing various opportunities on a path to medicine, yet this may not be a skill some individuals even see from their elders or peers if they grow up in a setting without business people or other professionals in their lives. It's a skill that can be developed, but this takes time, support, and a certain degree of trial-and-error that more initiated individuals will not have to go through.
Likewise, access to opportunities is far from equitable across individuals of different social status. One example that comes to mind is students who happen to have physicians as parents. These parents hear about or inquire about opportunities with their colleagues and provide a point of introduction for their children. These students must still show they are worthy of those opportunities and perform well once they secure them to advance further, but that first step is often a critical one. More importantly, opportunities create a snowball effect, where prior experience justifies acceptance to future opportunities, up to and including medical school. That is, individuals with higher social status and more connections can turn into seemingly more capable applicants - and may actually be more capable applicants - due to these connections, completely unrelated to ability or effort.
I'd like to emphasize that higher socioeconomic status does not remove the need for hard work or eliminate the role of a certain degree of natural ability in the process. Medicine, like many fields, is full of well-off individuals, but these people have nevertheless put in significant effort to get to where they are. However, what my recent experiences have reminded me of is that while hard work is necessary for success, it is not sufficient on its own, hence the title of this piece. Without trying to set up too much of a strawman, I think some well-off individuals give too much credit to their own hard work in achieving success, because they started to see success when they started putting in the effort. Yet these individuals started seeing success after they started to work harder towards success because everything else was already set up for them. I've met plenty of people who haven't had the same experience, where hard work perhaps improved their situations, but that improvement was limited due to factors beyond their control.
Bringing this back to the original point about the multifaceted nature of socioeconomic disadvantage for a minute, I now worry more that many interventions to improve such disadvantage are perhaps too simplistic to be effective. We can throw money at a problem but it can end up being a waste if the more social aspects to disadvantage are left unaddressed. On the flip side, we could try to improve these social elements, yet see minimal results if resources are still lacking. However, on a more positive note, this also means that there are many different ways we can make marginal improvements in peoples' lives. If we don't have money to help, we can volunteer time to teach new skills, or provide connections that might otherwise being lacking. If we're busy and running off our feet, financial supports can nevertheless be valuable. When people move up the socioeconomic ladder, patchwork systems of support like this can be an important reason why, allowing them to fully utilize their own natural talents and work ethic.
From a personal perspective, as I move forward within my own career in medicine, I'm hoping there will be more opportunities to level the playing field a little bit - and I hope I'll have the good sense to recognize when those opportunities arise.
Saturday, 20 May 2017
The Rise of Anti-Aging Technologies
Anti-aging technology is a relatively small, but rapidly-growing sector of research and development. Several research groups have been established, both in academia and in the corporate world. The corporate side is particularly interesting as venture capitalists are starting to throw money their way and even some big players, like Google, have directly entered the market. In Google's case, its start-up Calico, is clearly well-funded but shrouded in mystery, with little information provided publicly and seemingly few connections with academics or other companies working on anti-aging approaches.
It's an intriguing concept from a physician perspective, since our work is directly towards the extension and improvement of human lives, and age is a fairly significant non-modifiable risk factor in many, many diseases. Yet, it's hard to know what to make of these research efforts given the grandeur and complexity of the task, as well as the relative opaqueness of the field. So, I was glad to come across this interview with Aubrey de Grey, who rather passionately makes the case for continued anti-aging research, its plausibility, its potential, and then responds to societal critiques against the notion of anti-aging research entirely.
Dr de Grey's viewpoints provide an excellent window into the field of anti-aging research, but I admit to being a bit unconvinced on several of his points. First and foremost, on the technological side, there's promise, but in many cases, little more than that. One example Dr de Grey points to is the use of stem cells in degenerative diseases, like Parkinson's. While research on this issue is on-going and far from being exhausted, the promise of stem cell research has been touted for a few decades now without much success in reaching clinical treatments. I fully expect some breakthroughs in stem cell research, yet it's hard to have confidence that these will come soon, or that they will be as all-encompassing as has at times been promised. More likely, we'll see slow, incremental progress. Considering Dr de Grey's anti-aging framework requires such ambitious goals as effectively curing all major cancers - and I'd agree that's a necessity to substantially extend human life given that cancer incidence rises quickly with age - there's good reason to be skeptical that technologies are close to achieving his aims.
Regarding the societal critiques, namely inequality and overpopulation, I also feel the tone Dr de Grey sets is overly optimistic. For inequality, we already see fairly significant differences in access to healthcare based on cost. Any anti-aging costs stand to be rather expensive, if the level of investment in the potential anti-aging technologies is any indication. Even in a socialized healthcare system such as Canada's, this will be a concern. One example that springs to mind is the introduction of sofosbuvir (Sovaldi) for the treatment of Hepatitis C. It is a very expensive drug, but because it is so effective compared to previously-existing alternatives, it is actually a fairly cost-effective therapy by current metrics. Yet, provincial governments have been reluctant to fully-fund this drug due to its high cost. In Ontario, the sofosbuvir is only covered if a patient with Hepatitis C meets one of several requirements, even for those with provincially-funded drug plans, despite the indication for sofosbuvir being much more expansive than allowed for by these requirements. Even though sofosbuvir is effective and cost-effective, its upfront costs present a challenge for cash-strapped provinces. This is all for a drug that hits only a sliver of the population. Anti-aging drugs, which could in theory apply to everyone, will present much more a challenge, even if they work exactly as intended for a reasonable cost.
Overpopulation is, in my mind, a bit of a non-issue at this time since I'm skeptical anti-aging technologies will see widespread usage, but assuming they do, it becomes a serious concern. Dr de Grey notes that those who live longer can also contribute to society longer and thereby produce enough resources to justify their continued existence. This is absolutely true, but runs into problems when resources are constrained by more than manpower. Without starting down a whole different tangent, we are hitting the point where natural resources, which are independent of human work, are depleting far faster than they are being replaced. On top of this, we have a huge swath of humanity living on fewer resources than most of us would consider acceptable. While I believe this is a surmountable problem, it's not an easily-addressed one. Indeed, the world has been failing to adequately manage the shortcomings in our usage of natural resources relative to supply for decades at least, despite concerted efforts by many committed individuals, non-profits, and governments.
Lastly, an additional societal concern wasn't discussed in the article - the value of human turnover. That's a morbid thought, but our society relies on people moving onto new things, retiring from the workforce, or yes, even dying, in order to continue advancing forward. Older people carry with them older ideas and are more likely to have build up the power to implement them. Some of these are worth preserving. Others need to be let go. Longer life spans and longer careers means established ideas stay established longer, less pliable to the innovations of the young. Once again, this is a surmountable concern, and societies could adapt to a new normal of long-lived individuals, but I wouldn't be confident that this would be a seamless transition.
In short, I'm intrigued, but skeptical of this renewed anti-aging push. There are technical challenges that are far from simple to overcome. There are societal challenges that would have wide ranging impacts if not adequately addressed. Whether anti-aging efforts see success or failure, I'll be keeping my eye out for updates in this field.
It's an intriguing concept from a physician perspective, since our work is directly towards the extension and improvement of human lives, and age is a fairly significant non-modifiable risk factor in many, many diseases. Yet, it's hard to know what to make of these research efforts given the grandeur and complexity of the task, as well as the relative opaqueness of the field. So, I was glad to come across this interview with Aubrey de Grey, who rather passionately makes the case for continued anti-aging research, its plausibility, its potential, and then responds to societal critiques against the notion of anti-aging research entirely.
Dr de Grey's viewpoints provide an excellent window into the field of anti-aging research, but I admit to being a bit unconvinced on several of his points. First and foremost, on the technological side, there's promise, but in many cases, little more than that. One example Dr de Grey points to is the use of stem cells in degenerative diseases, like Parkinson's. While research on this issue is on-going and far from being exhausted, the promise of stem cell research has been touted for a few decades now without much success in reaching clinical treatments. I fully expect some breakthroughs in stem cell research, yet it's hard to have confidence that these will come soon, or that they will be as all-encompassing as has at times been promised. More likely, we'll see slow, incremental progress. Considering Dr de Grey's anti-aging framework requires such ambitious goals as effectively curing all major cancers - and I'd agree that's a necessity to substantially extend human life given that cancer incidence rises quickly with age - there's good reason to be skeptical that technologies are close to achieving his aims.
Regarding the societal critiques, namely inequality and overpopulation, I also feel the tone Dr de Grey sets is overly optimistic. For inequality, we already see fairly significant differences in access to healthcare based on cost. Any anti-aging costs stand to be rather expensive, if the level of investment in the potential anti-aging technologies is any indication. Even in a socialized healthcare system such as Canada's, this will be a concern. One example that springs to mind is the introduction of sofosbuvir (Sovaldi) for the treatment of Hepatitis C. It is a very expensive drug, but because it is so effective compared to previously-existing alternatives, it is actually a fairly cost-effective therapy by current metrics. Yet, provincial governments have been reluctant to fully-fund this drug due to its high cost. In Ontario, the sofosbuvir is only covered if a patient with Hepatitis C meets one of several requirements, even for those with provincially-funded drug plans, despite the indication for sofosbuvir being much more expansive than allowed for by these requirements. Even though sofosbuvir is effective and cost-effective, its upfront costs present a challenge for cash-strapped provinces. This is all for a drug that hits only a sliver of the population. Anti-aging drugs, which could in theory apply to everyone, will present much more a challenge, even if they work exactly as intended for a reasonable cost.
Overpopulation is, in my mind, a bit of a non-issue at this time since I'm skeptical anti-aging technologies will see widespread usage, but assuming they do, it becomes a serious concern. Dr de Grey notes that those who live longer can also contribute to society longer and thereby produce enough resources to justify their continued existence. This is absolutely true, but runs into problems when resources are constrained by more than manpower. Without starting down a whole different tangent, we are hitting the point where natural resources, which are independent of human work, are depleting far faster than they are being replaced. On top of this, we have a huge swath of humanity living on fewer resources than most of us would consider acceptable. While I believe this is a surmountable problem, it's not an easily-addressed one. Indeed, the world has been failing to adequately manage the shortcomings in our usage of natural resources relative to supply for decades at least, despite concerted efforts by many committed individuals, non-profits, and governments.
Lastly, an additional societal concern wasn't discussed in the article - the value of human turnover. That's a morbid thought, but our society relies on people moving onto new things, retiring from the workforce, or yes, even dying, in order to continue advancing forward. Older people carry with them older ideas and are more likely to have build up the power to implement them. Some of these are worth preserving. Others need to be let go. Longer life spans and longer careers means established ideas stay established longer, less pliable to the innovations of the young. Once again, this is a surmountable concern, and societies could adapt to a new normal of long-lived individuals, but I wouldn't be confident that this would be a seamless transition.
In short, I'm intrigued, but skeptical of this renewed anti-aging push. There are technical challenges that are far from simple to overcome. There are societal challenges that would have wide ranging impacts if not adequately addressed. Whether anti-aging efforts see success or failure, I'll be keeping my eye out for updates in this field.
Saturday, 13 May 2017
Initial Match Stats
The initial set of CaRMS stats was published recently, available here. As always, incomplete data means an incomplete interpretation, but there are some interesting take-aways.
First and foremost, it was a competitive match this year for CMGs, more so than it has been in recent years. More people going unmatched and fewer getting their preferred discipline or location. The changes from previous years are more marginal than dramatic, but there were indications that this year's competitiveness went beyond the typical year-to-year variation.
The reasons for this higher level of competitiveness are hard to definitively pin down, but two culprits present themselves. First, there are fewer residency spots relative to medical students. The ratio this year was the tightest it's been for decades, with the exception of last year, when it was slightly tighter. Without any other changes to the system, and none look to be incoming to alleviate the situation, this appears to be the new normal - a situation where the number of residency spots tracks very closely to the number of CMGs applying for those spots.
Second, there was a definite shift away from Family Medicine as a specialty of interest and towards both surgical specialties as well as Internal Medicine. Family Medicine is pretty much the only large specialty with more residency spots than there are demand for, while surgical specialties are almost always pursued by more students than they can accommodate. The change in interest in Internal is the real factor, however, as in the last two years it basically flipped from being a specialty with a small amount of room to accommodate more interested students to one that has too much interest relative to available spots. With Internal being the second-largest specialty, that's no small factor in the competitiveness of the match overall for CMGs.
While the full data set is necessary to draw lessons for future matches for CMGs, this early CaRMS presentation tends to provide the most useful information for IMGs. Of note here is that the number of IMGs rose for the first time since the NAC OSCE was made mandatory, particularly among first-time registrants. Many of them did not end up participating in the final match, as the IMG dropout rate is typically fairly high, but it signifies that we may start returning to the higher numbers of IMGs we saw before the mandatory NAC OSCE was introduced.
The CaRMS presentation shed some new light on the country-by-country results for IMG applicants. Those from English-speaking countries, who are typically Canadian students studying abroad, did better than most, with match rates in the 40-50% range. Those from the Caribbean, who are also typically Canadians studying abroad, did quite poorly, with match rates that appear to be in the mid-to-low teens. Those who graduated from other countries, often IMG who immigrated to Canada after completing medical school, had similarly poor match rates. The lesson here is clear - going to the UK, Ireland, or Australia offers notably better chances of matching to a residency in Canada, though the match rates are still no better than a coin toss.
Overall, the picture for residency matching appears bleaker, but again, the difference is marginal. Unlike last year when Ontario cut 25 residency spots, no major changes occurred in this year's match aside from shifts in student interest. The vast majority of CMGs still match and match high on their rank order lists. IMGs continue to face tough, but relatively stable odds. The trend, however, is not favourable and no relief appears to be in sight. The CaRMS match still largely works as intended, but the buffers that kept the system in place have been worn away to the point that relatively small changes - like a minor increase in interest in something like Internal Medicine - has the potential to cause outsized ripple effects.
First and foremost, it was a competitive match this year for CMGs, more so than it has been in recent years. More people going unmatched and fewer getting their preferred discipline or location. The changes from previous years are more marginal than dramatic, but there were indications that this year's competitiveness went beyond the typical year-to-year variation.
The reasons for this higher level of competitiveness are hard to definitively pin down, but two culprits present themselves. First, there are fewer residency spots relative to medical students. The ratio this year was the tightest it's been for decades, with the exception of last year, when it was slightly tighter. Without any other changes to the system, and none look to be incoming to alleviate the situation, this appears to be the new normal - a situation where the number of residency spots tracks very closely to the number of CMGs applying for those spots.
Second, there was a definite shift away from Family Medicine as a specialty of interest and towards both surgical specialties as well as Internal Medicine. Family Medicine is pretty much the only large specialty with more residency spots than there are demand for, while surgical specialties are almost always pursued by more students than they can accommodate. The change in interest in Internal is the real factor, however, as in the last two years it basically flipped from being a specialty with a small amount of room to accommodate more interested students to one that has too much interest relative to available spots. With Internal being the second-largest specialty, that's no small factor in the competitiveness of the match overall for CMGs.
While the full data set is necessary to draw lessons for future matches for CMGs, this early CaRMS presentation tends to provide the most useful information for IMGs. Of note here is that the number of IMGs rose for the first time since the NAC OSCE was made mandatory, particularly among first-time registrants. Many of them did not end up participating in the final match, as the IMG dropout rate is typically fairly high, but it signifies that we may start returning to the higher numbers of IMGs we saw before the mandatory NAC OSCE was introduced.
The CaRMS presentation shed some new light on the country-by-country results for IMG applicants. Those from English-speaking countries, who are typically Canadian students studying abroad, did better than most, with match rates in the 40-50% range. Those from the Caribbean, who are also typically Canadians studying abroad, did quite poorly, with match rates that appear to be in the mid-to-low teens. Those who graduated from other countries, often IMG who immigrated to Canada after completing medical school, had similarly poor match rates. The lesson here is clear - going to the UK, Ireland, or Australia offers notably better chances of matching to a residency in Canada, though the match rates are still no better than a coin toss.
Overall, the picture for residency matching appears bleaker, but again, the difference is marginal. Unlike last year when Ontario cut 25 residency spots, no major changes occurred in this year's match aside from shifts in student interest. The vast majority of CMGs still match and match high on their rank order lists. IMGs continue to face tough, but relatively stable odds. The trend, however, is not favourable and no relief appears to be in sight. The CaRMS match still largely works as intended, but the buffers that kept the system in place have been worn away to the point that relatively small changes - like a minor increase in interest in something like Internal Medicine - has the potential to cause outsized ripple effects.
Saturday, 6 May 2017
Survivorship in Medical Careers
It's been a while since I read XKCD, and stumbling across is recently reminded me why I should be reading it more regularly.
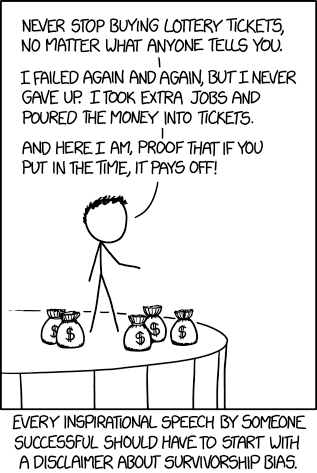
Source: XKCD (https://xkcd.com/1827/)
This is disturbingly relevant to those considering medicine, or those already in it. There are countless stories from people who have "made it", sharing their path to medicine and encouraging others to duplicate it. Some of these have merit. Many do not. The problem, as the XKCD comic notes, is the survivorship bias. There are many paths to and through medicine, but some are more risky than others. Those who achieve what could be considered to be a success naturally think they've got the inside track on how to become successful, because hey, it worked for them! I'm definitely guilty of this myself. Yet anecdotes are not data and what works for one person won't necessarily work for all people.
In medicine, the most common example of survivorship bias comes when considering attending medical school outside of Canada. It works for some people, people who are naturally pretty happy with the choice they made. Yet, we don't hear much from those who did not find success at a foreign medical school, who are understandably fairly shy about talking about their failures.
There are countless other situations where this holds true, however. There are many Canadian medical students who took some non-traditional paths to medicine. I did a second degree, for example. Others took comparatively difficult undergrads, such as engineering or art. Yet, while these paths work for some, I wouldn't call them reliable or optimal pathways to medicine.
I'd put CaRMS matching for Canadian medical students into this category as well. Successful candidates share their approach to matching to competitive programs, while those who didn't match, or matched low on their list generally don't share their often-very-similar stories.
The problem is that anecdotal data is often all students have to guide them. There isn't great data out there to say how to get into medical, how to land a good residency spot, or on the outcomes of studying medicine abroad. This is just my small reminder to treat every success story with a grain of salt, and to always, always, always have a reasonably reliable back-up plan in mind. Risk-taking is part of having a good career, as the only paths in life that come with guarantees are ones of mediocrity, yet gambling the future away in hopes of a payoff is never a recommended approach. Take the risks that still leave you standing if they don't work out - so that you can take the next chance that comes your way after that.
Saturday, 29 April 2017
Finances in Medicine - Big Life Expenses
As I move from student life to resident life, non-career life goals start to loom a little bit larger. At my age, many of my friends and colleagues are looking towards a few big expenses - getting a car, getting married, having kids, buying a house. None of these come cheap.
Car
This one's simple - most residencies require access to a vehicle, and in most cases, it's going to have to be your own vehicle. Buy something that fits your needs through residency that's reasonably low-maintenance (there's no time to be babying a fixer-upper). It shouldn't be a luxury vehicle. It'll likely be paid for through debt entirely and that's alright. It's a necessary business expense.
House
Ahh, the eternal debate - buy a house in residency or rent a place. In all honesty, there's no simple answer here, it'll depend on numerous factors. To the extent that there is any general advice, it's that the standard for Family Medicine residents is to rent, while the standard for those in 5-year specialties is to buy, but there are many exceptions to those guidelines.
The main reason to buy a house is to build equity with the money you're putting towards your living costs, thereby recouping some of that money rather than losing it as an expense outright. Buying a house becomes a forced investment - and a fairly good one at that - as the money paid towards a mortgage partially goes towards the house that you own, a house which is worth a lot of money and which will generally increase in price over time.
The main reason to rent is to avoid the costs and risks of homeownership. Spending money on rent is money that you'll never get back, but buying a house comes with its own expenses that will not be recouped. Maintenance, repairs, property taxes, interest (on the mortgage and, for residents, often on the down payment as well), closing costs, condo fees (if applicable) - all this adds up and is something renters don't need to deal with. Time is also a factor, as renting means that any housing issues that come up are the landlord's responsibility to deal with. Renting is also less risky, as houses can decline in value (but usually don't), and is more flexible if a move becomes necessary, as it often is for graduating residents.
All things considered, buying a house is usually a better financial decision in the long run. However, in the short-to-medium term, it comes with some distinct disadvantages. For those who have a little bit more medium term stability and a tolerance for some financial risk, it can be worthwhile. For those who face a bit more volatility in their upcoming housing needs or who are risk-averse, renting might be the better option and likely a bit cheaper in the short term. Regardless of the path chosen, all physicians will be able to afford a very nice property, likely a "forever home", only a few years after finishing residency - if not sooner.
Wedding
While everyone in residency needs transportation and housing, not everyone needs or wants to get married. Many do though, and the end of medical school is a prime time for it to happen. A good portion of my classmates just got married or have their wedding planned in the near future. Weddings, however, are expensive. Really expensive. Anything with a reception is likely to run at least $15k. More typical weddings are more in the $20-30k range. It's not hard to go above that upper end figure either. Oftentimes, these costs get offset by gifts from guests, either directly through money or through other gifts. Depending on the culture and attitudes of the guests, the entire cost of the wedding might be covered, but it's not something to count on either. For those uninterested in the traditional reception, a ceremony-only event is an option - whether it's the basic City Hall ceremony or a ceremony with more bells and whistles. The main cost of a wedding is the reception, and a very elegant ceremony can be funded for a fraction of the price of that reception.
Weddings are often financed by a combination of gifts, parental support, and debt. Fortunately, as a one-off event, most graduating medical students can afford that bit of extra debt without much difficulty. Still, when budgeting for the future, the expense of getting married should be in those calculations, because it is not a small one.
Children
Car
This one's simple - most residencies require access to a vehicle, and in most cases, it's going to have to be your own vehicle. Buy something that fits your needs through residency that's reasonably low-maintenance (there's no time to be babying a fixer-upper). It shouldn't be a luxury vehicle. It'll likely be paid for through debt entirely and that's alright. It's a necessary business expense.
House
Ahh, the eternal debate - buy a house in residency or rent a place. In all honesty, there's no simple answer here, it'll depend on numerous factors. To the extent that there is any general advice, it's that the standard for Family Medicine residents is to rent, while the standard for those in 5-year specialties is to buy, but there are many exceptions to those guidelines.
The main reason to buy a house is to build equity with the money you're putting towards your living costs, thereby recouping some of that money rather than losing it as an expense outright. Buying a house becomes a forced investment - and a fairly good one at that - as the money paid towards a mortgage partially goes towards the house that you own, a house which is worth a lot of money and which will generally increase in price over time.
The main reason to rent is to avoid the costs and risks of homeownership. Spending money on rent is money that you'll never get back, but buying a house comes with its own expenses that will not be recouped. Maintenance, repairs, property taxes, interest (on the mortgage and, for residents, often on the down payment as well), closing costs, condo fees (if applicable) - all this adds up and is something renters don't need to deal with. Time is also a factor, as renting means that any housing issues that come up are the landlord's responsibility to deal with. Renting is also less risky, as houses can decline in value (but usually don't), and is more flexible if a move becomes necessary, as it often is for graduating residents.
All things considered, buying a house is usually a better financial decision in the long run. However, in the short-to-medium term, it comes with some distinct disadvantages. For those who have a little bit more medium term stability and a tolerance for some financial risk, it can be worthwhile. For those who face a bit more volatility in their upcoming housing needs or who are risk-averse, renting might be the better option and likely a bit cheaper in the short term. Regardless of the path chosen, all physicians will be able to afford a very nice property, likely a "forever home", only a few years after finishing residency - if not sooner.
Wedding
While everyone in residency needs transportation and housing, not everyone needs or wants to get married. Many do though, and the end of medical school is a prime time for it to happen. A good portion of my classmates just got married or have their wedding planned in the near future. Weddings, however, are expensive. Really expensive. Anything with a reception is likely to run at least $15k. More typical weddings are more in the $20-30k range. It's not hard to go above that upper end figure either. Oftentimes, these costs get offset by gifts from guests, either directly through money or through other gifts. Depending on the culture and attitudes of the guests, the entire cost of the wedding might be covered, but it's not something to count on either. For those uninterested in the traditional reception, a ceremony-only event is an option - whether it's the basic City Hall ceremony or a ceremony with more bells and whistles. The main cost of a wedding is the reception, and a very elegant ceremony can be funded for a fraction of the price of that reception.
Weddings are often financed by a combination of gifts, parental support, and debt. Fortunately, as a one-off event, most graduating medical students can afford that bit of extra debt without much difficulty. Still, when budgeting for the future, the expense of getting married should be in those calculations, because it is not a small one.
Children
As with weddings, many people are opting not to have children, so this may be a non-issue for a growing number of physicians. For those that want kids, children require some serious financial planning. The cost of raising a child to adulthood averages over $250k in Canada, with expenses being higher in the early years. For physicians with generally high standards of living and above-average expectations for their children's care, that figure is likely an underestimate. That's a significant and continuous cost to bear.
Perhaps most challenging for those in medicine, children can't always be put off until later, while houses and weddings can be delayed indefinitely. The biological clock is an unavoidable fact of life for a career path that requires training into many physicians' early 30's or beyond. Women in medicine unquestionably bear the brunt of this reality more so than men, though men are not exempt from timelines either when it comes to having children. Timing therefore becomes a rather important decision. The longer physicians wait to have children, the more financially secure they'll be, but the older they'll be before trying to conceive or adopt.
A small number choose to have children in medical school. Time-wise, this can be a good option. Outside of clerkship, schedules are much lighter and more flexible than they are in residency. Medical schools often do allow time off for children, though this typical means being kept back a year and may mean an extra year of tuition payments. Medical students are, naturally, quite young as well. Money is an issue though, as medical students are piling on debt, not bringing in an income. Within reason, debt-financing child expenses can be done. However, other expenses will have to be kept under tight control unless a high-earning partner is in the picture, and careful financial management is a must.
Waiting until becoming an attending physician is a more common time frame to start having children. By this point demands on physician time have (usually) settled down and are much more flexible. There should be plenty of financial resources available by this point as well. The downsides are age and the hassle of practice management. Age is fairly self-explanatory when it comes to waiting until after residency, but practice management is an often-neglected factor. Unlike in medical school and residency, attending physicians are now fully responsible for their own careers. Taking time off to have a child means, in many cases, having to find someone to cover your practice. This can be particularly worrisome immediately post-residency, when a physician is still working to establish themselves and may not be able to easily take time off just yet. These immediate post-residency career demands can push the timeline to have children back even further than intended. Still, for those who are on the younger side, in shorter residency programs, or happy with being on the older side to start trying, waiting until after residency can be a rather sensible choice.
At the end of the day, residency remains a very popular time to start having children. Time is in exceedingly short supply, but taking maternity or paternity leave is relatively straight-forward. Residents aren't exactly overflowing with money, but they've got enough coming in to support a household. They're older than medical students, but younger than attendings, most being in their late-20's or early-30's, which is a fairly favourable time to start having kids. Residency remains the standard "recommended" time to have children for these reasons.
Nevertheless, circumstances will be different for every individual physician, and there are certainly merits to starting to have children either before or after residency. The timing of having children is a balancing act of competing priorities, and any decision will involve some trade-offs. Proper financial planning and lifestyle management remain the greatest assets when considering children.
Perhaps most challenging for those in medicine, children can't always be put off until later, while houses and weddings can be delayed indefinitely. The biological clock is an unavoidable fact of life for a career path that requires training into many physicians' early 30's or beyond. Women in medicine unquestionably bear the brunt of this reality more so than men, though men are not exempt from timelines either when it comes to having children. Timing therefore becomes a rather important decision. The longer physicians wait to have children, the more financially secure they'll be, but the older they'll be before trying to conceive or adopt.
A small number choose to have children in medical school. Time-wise, this can be a good option. Outside of clerkship, schedules are much lighter and more flexible than they are in residency. Medical schools often do allow time off for children, though this typical means being kept back a year and may mean an extra year of tuition payments. Medical students are, naturally, quite young as well. Money is an issue though, as medical students are piling on debt, not bringing in an income. Within reason, debt-financing child expenses can be done. However, other expenses will have to be kept under tight control unless a high-earning partner is in the picture, and careful financial management is a must.
Waiting until becoming an attending physician is a more common time frame to start having children. By this point demands on physician time have (usually) settled down and are much more flexible. There should be plenty of financial resources available by this point as well. The downsides are age and the hassle of practice management. Age is fairly self-explanatory when it comes to waiting until after residency, but practice management is an often-neglected factor. Unlike in medical school and residency, attending physicians are now fully responsible for their own careers. Taking time off to have a child means, in many cases, having to find someone to cover your practice. This can be particularly worrisome immediately post-residency, when a physician is still working to establish themselves and may not be able to easily take time off just yet. These immediate post-residency career demands can push the timeline to have children back even further than intended. Still, for those who are on the younger side, in shorter residency programs, or happy with being on the older side to start trying, waiting until after residency can be a rather sensible choice.
At the end of the day, residency remains a very popular time to start having children. Time is in exceedingly short supply, but taking maternity or paternity leave is relatively straight-forward. Residents aren't exactly overflowing with money, but they've got enough coming in to support a household. They're older than medical students, but younger than attendings, most being in their late-20's or early-30's, which is a fairly favourable time to start having kids. Residency remains the standard "recommended" time to have children for these reasons.
Nevertheless, circumstances will be different for every individual physician, and there are certainly merits to starting to have children either before or after residency. The timing of having children is a balancing act of competing priorities, and any decision will involve some trade-offs. Proper financial planning and lifestyle management remain the greatest assets when considering children.
Saturday, 22 April 2017
Finances in Medicine - Insurance
Having money, or the potential to make money, comes with the unfortunate flip-side of having the potential to lose money. A lot of money. That's where insurance comes in. There are a plethora of insurance types and options within those types, which become tricky to sort out. They can also be very expensive. In the last couple months, this is where I've been spending a lot of mental energy, trying to sort out the optimal insurance balance.
Disability Insurance
Disability insurance is required for 99% of people. The only people who shouldn't buy disability insurance are those who could afford to retire right this second and be completely financially secure. At this stage, this pretty much just means people who are independently wealthy. For those near the end of their careers, who are continuing to work out of interest more than financial need, and have their retirement amply well-financed, disability insurance might also be worthwhile to stop purchasing, since those individuals can simply retire in the event of a disability.
Physicians have high current or future incomes, but those incomes require us to be able to work. If we can't work, we lose that income and, in many cases, are stuck with a lot of debt or an unaffordable lifestyle. Disability insurance means that if you can't work, you can still live comfortably while you recover or transition out of the workforce entirely. You should have as much of it as possible, as soon as possible, so that your income stays as close to your working income if you become disabled. Insurers are smart though, and realize that if workers can get paid as much or more than they currently do if they become disabled, it provides a strong incentive to become disabled, so no insurer will give you disability insurance that covers your full income. The immediate thought then is to get multiple lines of disability insurance, but insurers are one step ahead there too - they'll only pay out a maximum amount collectively, meaning that if you have $X amount of coverage with one insurer and $Y amount of coverage with another insurer, you won't get $X+Y in payouts, you'll get whichever of $X or $Y is higher. That usually means it makes sense to have only a single disability insurance provider.
The first disability insurance most of us will be offered is through our provincial medical associations. In Ontario, the OMA offers rather cheap disability insurance to medical students without a medical, which is worthwhile to take. There are some private options, but they're unlikely to be advantageous in terms of cost, so sticking with the association insurance through medical school is fine for most people. Once in residency, the landscape changes slightly. Association insurance continues to be quite cheap and is generally worth maintaining through residency. However, in most provinces, residency comes with an automatic, employer-provided disability insurance that lasts through residency. It's not terribly great insurance, relatively speaking, and it goes away as soon as residency is done, but it's mandatory. One big advantage with these mandatory, employer-provided disability insurance plans is that in Ontario at least, their benefits are not mutually exclusive with the association coverage. Residency basically breaks the rule that says disability should not be profitable above current salary, though the benefits are still far less than what a fully-qualified physician should make.
Once residency finishes, association plans become expensive, opening up the door for privately provided disability insurance. These private plans aren't cheaper per se, but they come with one major advantage - guarantees. Association plans are owned by the association. Their fees could change, their benefits could change, and you as a client cannot stop it individually. Associations do work on behalf of their members and therefore do not have much cause to agree to a worse deal. If anything, provincial medical associations tend to improve the terms of their deals over time, so this problem is more theoretical than real. Yet, private plans are owned by you, individually, and cannot change for any reason whatsoever. Fees won't change, benefits won't change, nothing can change. The downside of private plans is that they typically require a medical, which could result in higher rates, and will require a year or two of payments before any pre-existing conditions are covered. This simply means that a period of crossover with the association plans is necessary to ensure continuous disability coverage. At this point association vs private insurance is a matter of preference and comfort, mostly between the guaranteed association coverage that does not necessarily require a medical, or private insurance that does not require faith in the provincial medical association to behave appropriately.
Life Insurance
At some point, you will die. That'll suck. If you die before you retire, you may leave behind some people who were relying on you to earn money. This can be a spouse, stuck with your student debt or a mortgage, children who were counting on you to provide for their future, or other dependents like elderly parents who need some financial help in their day-to-day lives. If you have any of these people in your life, you need life insurance. If you don't, you probably don't need life insurance.
Once again, in Ontario, the OMA provides life insurance for students, this time for free, and it's perfectly adequate for medical school for pretty much anyone who does not have children or other dependents. Life insurance is otherwise pretty independent of stage of training. You need some, it doesn't particularly matter who provides it, as long as it covers whatever costs you'd need to cover in the event of your death. It should be term life insurance, which is generally cheap and expires after a set period of time, at which point you can buy insurance for another term (if you need it). It'll generally be more expensive when you renew because you're older and more likely to die at that point, but that's pretty much unavoidable.
There are other forms of life insurance which can technically last forever, meaning they'll pay out eventually, but they're expensive and generally not worthwhile. They cost you more when you're alive than they'll pay to your estate when you die - you might as well just save that money and invest it. Insurance is meant to lose you money, on average, to guard against an unlikely-but-disastrous outcome. Dying young, which is unlikely, is exactly what insurance is meant for. Dying ever, which is 100% going to happen, is not what insurance is meant for.
Home and Auto Insurance
Do you have a home? A car? Buy insurance for them. They're expensive and you need them.
Other Insurance
There's insurance for just about anything. It comes in all shapes, sizes, costs, and terms. You don't need most of it. You might need some of it, depending on circumstances. In general, you should have insurance for anything expensive you own that you couldn't afford to replace if it got destroyed. That includes yourself. Disability and life insurance cover the "you" part pretty well, but supplementary health insurance might be worthwhile too. Home and auto insurance cover your major personal assets, but you may have other personal property to protect, as well as professional assets such as office space. These individual needs should be discussed with a professional and considered with the following question in mind - can I easily afford to lose the thing I am insuring? If you can, insurance probably isn't necessary. If you can't, it probably is.
One important "other" insurance to mention is insurance on debt. This can be insurance on a line of credit, on a credit card, or on a mortgage. Avoid this insurance like the plague. This type of insurance protects the bank in the event you default on your loan. It's for the bank's benefit, not your's. The guard for yourself against defaulting on these loans is the disability and life insurance you should already have. That's there for you, it goes to you, and it should cover your debts.
Yikes this post got long. Insurance is important, but my apologies for rambling! I will follow-up with some hopefully-shorter thoughts on planning major life expenses to wrap up this impromptu series on finances.
Disability Insurance
Disability insurance is required for 99% of people. The only people who shouldn't buy disability insurance are those who could afford to retire right this second and be completely financially secure. At this stage, this pretty much just means people who are independently wealthy. For those near the end of their careers, who are continuing to work out of interest more than financial need, and have their retirement amply well-financed, disability insurance might also be worthwhile to stop purchasing, since those individuals can simply retire in the event of a disability.
Physicians have high current or future incomes, but those incomes require us to be able to work. If we can't work, we lose that income and, in many cases, are stuck with a lot of debt or an unaffordable lifestyle. Disability insurance means that if you can't work, you can still live comfortably while you recover or transition out of the workforce entirely. You should have as much of it as possible, as soon as possible, so that your income stays as close to your working income if you become disabled. Insurers are smart though, and realize that if workers can get paid as much or more than they currently do if they become disabled, it provides a strong incentive to become disabled, so no insurer will give you disability insurance that covers your full income. The immediate thought then is to get multiple lines of disability insurance, but insurers are one step ahead there too - they'll only pay out a maximum amount collectively, meaning that if you have $X amount of coverage with one insurer and $Y amount of coverage with another insurer, you won't get $X+Y in payouts, you'll get whichever of $X or $Y is higher. That usually means it makes sense to have only a single disability insurance provider.
The first disability insurance most of us will be offered is through our provincial medical associations. In Ontario, the OMA offers rather cheap disability insurance to medical students without a medical, which is worthwhile to take. There are some private options, but they're unlikely to be advantageous in terms of cost, so sticking with the association insurance through medical school is fine for most people. Once in residency, the landscape changes slightly. Association insurance continues to be quite cheap and is generally worth maintaining through residency. However, in most provinces, residency comes with an automatic, employer-provided disability insurance that lasts through residency. It's not terribly great insurance, relatively speaking, and it goes away as soon as residency is done, but it's mandatory. One big advantage with these mandatory, employer-provided disability insurance plans is that in Ontario at least, their benefits are not mutually exclusive with the association coverage. Residency basically breaks the rule that says disability should not be profitable above current salary, though the benefits are still far less than what a fully-qualified physician should make.
Once residency finishes, association plans become expensive, opening up the door for privately provided disability insurance. These private plans aren't cheaper per se, but they come with one major advantage - guarantees. Association plans are owned by the association. Their fees could change, their benefits could change, and you as a client cannot stop it individually. Associations do work on behalf of their members and therefore do not have much cause to agree to a worse deal. If anything, provincial medical associations tend to improve the terms of their deals over time, so this problem is more theoretical than real. Yet, private plans are owned by you, individually, and cannot change for any reason whatsoever. Fees won't change, benefits won't change, nothing can change. The downside of private plans is that they typically require a medical, which could result in higher rates, and will require a year or two of payments before any pre-existing conditions are covered. This simply means that a period of crossover with the association plans is necessary to ensure continuous disability coverage. At this point association vs private insurance is a matter of preference and comfort, mostly between the guaranteed association coverage that does not necessarily require a medical, or private insurance that does not require faith in the provincial medical association to behave appropriately.
Life Insurance
At some point, you will die. That'll suck. If you die before you retire, you may leave behind some people who were relying on you to earn money. This can be a spouse, stuck with your student debt or a mortgage, children who were counting on you to provide for their future, or other dependents like elderly parents who need some financial help in their day-to-day lives. If you have any of these people in your life, you need life insurance. If you don't, you probably don't need life insurance.
Once again, in Ontario, the OMA provides life insurance for students, this time for free, and it's perfectly adequate for medical school for pretty much anyone who does not have children or other dependents. Life insurance is otherwise pretty independent of stage of training. You need some, it doesn't particularly matter who provides it, as long as it covers whatever costs you'd need to cover in the event of your death. It should be term life insurance, which is generally cheap and expires after a set period of time, at which point you can buy insurance for another term (if you need it). It'll generally be more expensive when you renew because you're older and more likely to die at that point, but that's pretty much unavoidable.
There are other forms of life insurance which can technically last forever, meaning they'll pay out eventually, but they're expensive and generally not worthwhile. They cost you more when you're alive than they'll pay to your estate when you die - you might as well just save that money and invest it. Insurance is meant to lose you money, on average, to guard against an unlikely-but-disastrous outcome. Dying young, which is unlikely, is exactly what insurance is meant for. Dying ever, which is 100% going to happen, is not what insurance is meant for.
Home and Auto Insurance
Do you have a home? A car? Buy insurance for them. They're expensive and you need them.
Other Insurance
There's insurance for just about anything. It comes in all shapes, sizes, costs, and terms. You don't need most of it. You might need some of it, depending on circumstances. In general, you should have insurance for anything expensive you own that you couldn't afford to replace if it got destroyed. That includes yourself. Disability and life insurance cover the "you" part pretty well, but supplementary health insurance might be worthwhile too. Home and auto insurance cover your major personal assets, but you may have other personal property to protect, as well as professional assets such as office space. These individual needs should be discussed with a professional and considered with the following question in mind - can I easily afford to lose the thing I am insuring? If you can, insurance probably isn't necessary. If you can't, it probably is.
One important "other" insurance to mention is insurance on debt. This can be insurance on a line of credit, on a credit card, or on a mortgage. Avoid this insurance like the plague. This type of insurance protects the bank in the event you default on your loan. It's for the bank's benefit, not your's. The guard for yourself against defaulting on these loans is the disability and life insurance you should already have. That's there for you, it goes to you, and it should cover your debts.
Yikes this post got long. Insurance is important, but my apologies for rambling! I will follow-up with some hopefully-shorter thoughts on planning major life expenses to wrap up this impromptu series on finances.
Saturday, 15 April 2017
Finances in Medicine
Reaching the end of my final year of medical school, suddenly money has become very important. My student debt levels are reaching their maximum, but I'm about to start earning a real salary for the first time since I left my previous career to start medical school four years ago. With that comes a chance to move on to the next stages in life, as well as an obligation to start contributing financially to society at large, after having largely been a sponge for my life up until now.
Education on medical trainee finances, despite being rather unique and complex, is still largely lacking, and mostly coming from people who have a financial stake it your decisions. Most advisers are reasonably honest and up-front about the rationale behind their recommendations - true shysters get driven out of the industry fairly quickly - but sorting out what's best for you isn't always easy. Here's what I've found out so far.
Debt Management
Naturally, this starts in or even before the first year of medical school, when debt starts to build. Just a quick reminder of the basics, the ideal approach is to maximize scholarships/bursaries/grants first (free money!), then maximize government loans (usually come with no interest while studying, many have grants attached), then rely on private loans in the form of a line of credit (LOC) specific to medical students. Once residency comes and government loans start generating interest, usually at a higher rate than LOCs, it's best to roll the entire sum of the government loans into the LOC, unless you qualify for certain governmental debt-relief programs that require you to leave a balance in those government loans to take advantage of them. There are some individuals who, through bursaries or other outside funding, can get through medical school with just government loans.
Some money can be earned by working in medical school by working. Since government loans and grants get reduced by personal income, however, there are significant diminishing returns on getting a job. Some jobs - such as research positions - can be worthwhile even if they were paid nothing, and so earning money from them is just a small extra benefit. Jobs that are taken just for the money may not be worthwhile, however, as it's not hard to be in a position where a student is working for far less than minimum wage once lost governmental grants are taken into account.
Once in residency and earning a real salary, debt can start to be paid down, though it does not have to be. Depending on personal circumstances, some people will build on their debt, some will keep it stable by paying off any generated interest, others will reduce their debt significantly. For the most part, however, now is when debt-paying habits can start in earnest, even if it is just covering the interest. Automatic transfers are ideal, since it's very easy to upgrade lifestyle to match income if that money is perceived to be available. Developing these habits now is mostly important to carry on into post-residency life, as debt-repayment strategies are pretty much identical to the basic savings strategies which define whether a physician is financially secure or has constant money troubles.
Throughout medical school and into residency, the best thing a trainee can do for their debt is to keep it low by controlling spending. Living a modest lifestyle, even when you can technically afford more, makes future financial decisions significantly easier. Living in a smaller place, eating out less, forgoing nice but unnecessary luxuries, and ultimately, budgeting to keep costs low is how to succeed financially. As with debt repayment, forming the habit that spending is to be deliberate and well below one's means is the most critical aspect. Many physicians have financial troubles and for 99% of them, it's a problem of uncontrolled spending. Learning how to avoid those problems early on, in medical school and residency when it still has a large impact on overall debt load, is an important skill.
There's a lot more financial stuff on my mind these days, but this post started getting a little out of hand, so I'll split it into parts. Best advice I can give to those looking to revamp their finances is to get informed and tailor their approach to their own situation. There's some good advice there, but rarely a one-size-fits-all approach. Money management is not something that can be outsourced, medical students, residents, and physicians need to take an active and informed role in their own finances.
Education on medical trainee finances, despite being rather unique and complex, is still largely lacking, and mostly coming from people who have a financial stake it your decisions. Most advisers are reasonably honest and up-front about the rationale behind their recommendations - true shysters get driven out of the industry fairly quickly - but sorting out what's best for you isn't always easy. Here's what I've found out so far.
Debt Management
Naturally, this starts in or even before the first year of medical school, when debt starts to build. Just a quick reminder of the basics, the ideal approach is to maximize scholarships/bursaries/grants first (free money!), then maximize government loans (usually come with no interest while studying, many have grants attached), then rely on private loans in the form of a line of credit (LOC) specific to medical students. Once residency comes and government loans start generating interest, usually at a higher rate than LOCs, it's best to roll the entire sum of the government loans into the LOC, unless you qualify for certain governmental debt-relief programs that require you to leave a balance in those government loans to take advantage of them. There are some individuals who, through bursaries or other outside funding, can get through medical school with just government loans.
Some money can be earned by working in medical school by working. Since government loans and grants get reduced by personal income, however, there are significant diminishing returns on getting a job. Some jobs - such as research positions - can be worthwhile even if they were paid nothing, and so earning money from them is just a small extra benefit. Jobs that are taken just for the money may not be worthwhile, however, as it's not hard to be in a position where a student is working for far less than minimum wage once lost governmental grants are taken into account.
Once in residency and earning a real salary, debt can start to be paid down, though it does not have to be. Depending on personal circumstances, some people will build on their debt, some will keep it stable by paying off any generated interest, others will reduce their debt significantly. For the most part, however, now is when debt-paying habits can start in earnest, even if it is just covering the interest. Automatic transfers are ideal, since it's very easy to upgrade lifestyle to match income if that money is perceived to be available. Developing these habits now is mostly important to carry on into post-residency life, as debt-repayment strategies are pretty much identical to the basic savings strategies which define whether a physician is financially secure or has constant money troubles.
Throughout medical school and into residency, the best thing a trainee can do for their debt is to keep it low by controlling spending. Living a modest lifestyle, even when you can technically afford more, makes future financial decisions significantly easier. Living in a smaller place, eating out less, forgoing nice but unnecessary luxuries, and ultimately, budgeting to keep costs low is how to succeed financially. As with debt repayment, forming the habit that spending is to be deliberate and well below one's means is the most critical aspect. Many physicians have financial troubles and for 99% of them, it's a problem of uncontrolled spending. Learning how to avoid those problems early on, in medical school and residency when it still has a large impact on overall debt load, is an important skill.
There's a lot more financial stuff on my mind these days, but this post started getting a little out of hand, so I'll split it into parts. Best advice I can give to those looking to revamp their finances is to get informed and tailor their approach to their own situation. There's some good advice there, but rarely a one-size-fits-all approach. Money management is not something that can be outsourced, medical students, residents, and physicians need to take an active and informed role in their own finances.
Wednesday, 5 April 2017
CaRMS & Match Strategies
My class got a quick and by no means thorough breakdown of our overall match results, where the most notable highlight was a complimentary breakfast ten times better than anything I'd been served throughout the prior 4 years. The other notable point concerned how our class did in the match. I'll pump up my cohorts here a bit - we had a lot of people match to some rather competitive specialties, especially surgical specialties. Otherwise our results were fairly typical for our school in terms of the overall unmatched. There's some very good soon-to-be physicians in that cohort of unmatched people at my school, so I'm really hoping they land somewhere acceptable in the second round, or match to their intended residency next year if nothing suitable is left available this year.
Getting a chance to be a bit more up-close-and-personal to the match process has reinforced a few things I had been told, as well as a few I hadn't thought of, when it comes to match strategy.
First and foremost, a good match strategy - applying broadly, backing up where it makes sense to - is still absolutely the way to go. Beggars can't be choosers and when it comes to CaRMS, we're all beggars.
Second, and a perhaps slight caveat to the first, elective choices matter. Splitting electives between competitive specialties is a great way to get neither. The odd person may be able to pull it off, but it's a gamble, even for well-qualified individuals. Backing up should be done when possible, but if a candidate can't give themselves a desirable, viable back-up option without significantly hurting their chances with their first-choice specialty, then maybe a back-up no longer makes sense. Programs shouldn't care about a candidate's exclusive interest in their specialty - the CaRMS algorithm is meant precisely to avoid that kind of thinking - but they do and it shows. Even for less competitive specialties, not showing a reasonable commitment can be a detriment to matching. Any elective set-up should be purposefully created, with a logic to it that fits with a reasonable set of match goals, taking into consideration the timing of CaRMS, the specialty or specialties being applied to, and any geographical restrictions.
Third, networking and playing the social game absolutely have an impact, particularly in smaller fields. Moreover, that factor may be justified. While we often want people to get ahead based on ability than who likes them, few jobs are performed in isolation and medicine is definitely a social job. An ability to get along with others amicably makes a difference in terms of the functioning of the whole group. Networking and playing the social game are the ways to prove that you're easy enough to get along with. Building off the prior point, electives are the ultimate networking opportunity, which is part of the reason they're so important.
Lastly, chance is still a huge factor. In any CaRMS cycle, there seems to be a set of individuals who are phenomenal, clearly desired by programs, and are near-locks to match. That they land their first-choice programs is no surprise. On the opposite end, there are a very small number of individuals who are unsurprisingly left unmatched, or who in some cases never make it through medical school to the match. Yet, most of us fall into the vast middle ground, where we're good, competent candidates without standing head-and-shoulders above the rest. There are differences between candidates in this substantial middle-of-the-pack group, certainly, but the differences end up being more like a difference in flavour than in quality. As a result, when someone ends up on the outside looking in after the first iteration, luck plays a significant role. With the match overall being more competitive than it has been in the past, someone has to go unmatched and it very often is someone who really didn't do anything wrong. Unfortunately people who go unmatched in the first round, or their first year, face a stigma of inferiority, one which is not deserved in many cases. I think this is the part of the CaRMS match that really hit home this year - while the way we approach our residency match does involve some merit-based stratification, outside the extremes it's far less about merit than we like to believe.
Overall, my feelings on a good approach to a match haven't changed much, but the overall importance of certain aspects has. I'm lucky to have had the outcome I did. If I had any new advice to give prospective residents, it'd be merely to emphasize the importance of being proactive with their electives and with developing contacts. Otherwise, stick to the tried-and-true strategies, they're standards for a reason.
Getting a chance to be a bit more up-close-and-personal to the match process has reinforced a few things I had been told, as well as a few I hadn't thought of, when it comes to match strategy.
First and foremost, a good match strategy - applying broadly, backing up where it makes sense to - is still absolutely the way to go. Beggars can't be choosers and when it comes to CaRMS, we're all beggars.
Second, and a perhaps slight caveat to the first, elective choices matter. Splitting electives between competitive specialties is a great way to get neither. The odd person may be able to pull it off, but it's a gamble, even for well-qualified individuals. Backing up should be done when possible, but if a candidate can't give themselves a desirable, viable back-up option without significantly hurting their chances with their first-choice specialty, then maybe a back-up no longer makes sense. Programs shouldn't care about a candidate's exclusive interest in their specialty - the CaRMS algorithm is meant precisely to avoid that kind of thinking - but they do and it shows. Even for less competitive specialties, not showing a reasonable commitment can be a detriment to matching. Any elective set-up should be purposefully created, with a logic to it that fits with a reasonable set of match goals, taking into consideration the timing of CaRMS, the specialty or specialties being applied to, and any geographical restrictions.
Third, networking and playing the social game absolutely have an impact, particularly in smaller fields. Moreover, that factor may be justified. While we often want people to get ahead based on ability than who likes them, few jobs are performed in isolation and medicine is definitely a social job. An ability to get along with others amicably makes a difference in terms of the functioning of the whole group. Networking and playing the social game are the ways to prove that you're easy enough to get along with. Building off the prior point, electives are the ultimate networking opportunity, which is part of the reason they're so important.
Lastly, chance is still a huge factor. In any CaRMS cycle, there seems to be a set of individuals who are phenomenal, clearly desired by programs, and are near-locks to match. That they land their first-choice programs is no surprise. On the opposite end, there are a very small number of individuals who are unsurprisingly left unmatched, or who in some cases never make it through medical school to the match. Yet, most of us fall into the vast middle ground, where we're good, competent candidates without standing head-and-shoulders above the rest. There are differences between candidates in this substantial middle-of-the-pack group, certainly, but the differences end up being more like a difference in flavour than in quality. As a result, when someone ends up on the outside looking in after the first iteration, luck plays a significant role. With the match overall being more competitive than it has been in the past, someone has to go unmatched and it very often is someone who really didn't do anything wrong. Unfortunately people who go unmatched in the first round, or their first year, face a stigma of inferiority, one which is not deserved in many cases. I think this is the part of the CaRMS match that really hit home this year - while the way we approach our residency match does involve some merit-based stratification, outside the extremes it's far less about merit than we like to believe.
Overall, my feelings on a good approach to a match haven't changed much, but the overall importance of certain aspects has. I'm lucky to have had the outcome I did. If I had any new advice to give prospective residents, it'd be merely to emphasize the importance of being proactive with their electives and with developing contacts. Otherwise, stick to the tried-and-true strategies, they're standards for a reason.
Thursday, 30 March 2017
Addiction and Physicians - Why Having an MD Doesn't Make You Special
Haven't posted much lately, though not necessarily by intention. Life's been very crazy lately, but in a very good way.
Wanted to touch on a story that's rightfully making the rounds on social media, of a Canadian physician talking about his addiction to Fentanyl. Fentanyl is the new addict drug of choice in much of Canada, particularly in southern Ontario. It's been building for a few years. Every conversation I have with those in addictions or drug enforcement says that this is where we're seeing a big focus. It's a very powerful narcotic, one that's definitely overprescribed, and it has numerous routes of absorption. In many ways, it's the most recent culmination of the wider opioid crisis that's been growing for decades now.
Dr Gebien's tale is worth reading for its account of the devastating effects of opioid addiction, and the hubris of physicians who think they're immune to such common human failings. On the former point, there's enough written by more knowledgeable people than me that I won't say much besides a reiteration that I want my practice to be very opioid-averse. As far as I'm concerned, unless something's going to cure your pain very soon (usually by an operation of some sort), or we expect you to die at some point in the near future, I have trouble seeing the role of opioids. They don't work well long term, they're addictive, and they come with tons of side-effects. They're not really a treatment for pain, they're a way to stall it in the short-term.
On the second point, it can't be emphasized enough - doctors are human and we fall victim to all the things humans fall victim to, including addiction. One particular point to mention about this story is the hazards of self-prescribing. Physicians are not supposed to treat anyone who isn't their patient, including themselves. That means no treating family or friends except in very unique circumstances. That means no treating co-workers. That means no treating fellow physicians unless they're in your office for a valid reason. I can't say how often I've seen a physician write off a prescription to one of their colleagues based on that colleague's word alone. No history. No physical. No investigations. Just "I need this script, can you help me out?", and bam, done. In one instance, a physician asked a colleague for a medication for their child, effectively treating their own kid with the help of a fellow physician who never even laid eyes on that child! Don't do this. Yes, it sucks to have to go to your GP to get a simple script. Yes, you know exactly what needs to be done. You know who else it sucks for to have to do that? EVERYONE! Being a physician should not get you a fast track to basic medical care, nor should it allow you to skip the basic components of treatment, such as a proper evaluation. Please, colleagues, supervisors, and anyone coming afterwards, just don't do this, and don't help others do this. It's unethical and can lead to some very dark outcomes.
There's a few other elements to this story that deserve a quick mention, since they probably contributed to his situation and are much more common traps for physicians to fall into then addiction. First is proper money management. He was making $300k a year and needed parental assistance to cover two rehab-related bills of $10k and $80k, in addition to needing to put $35k on a line-of-credit. Everyone, regardless of profession, should have an Emergency fund of at least 6 months of living expenses, ideally 1 year's worth. In his case, it doesn't sound like he had anywhere close to that. I don't doubt that a fair bit of money was going to feed or hide is addiction. Yet, there are other clear missteps. Buying a large house, luxury cars, and a boat weren't necessary and probably weren't affordable. Even if your means are great, you still need to live within them.
Secondly, this story highlights the need for a robust support system. Here we see only one side of the story, so it's hard to draw conclusions, but I don't get the sense of a reliable base of support from Dr Gebien's wife or parents. Their relationships seem dysfunctional and his mother, who looked to be dealing with her own problems of opioid use, was an enabler in his addiction. Building connections with reliable people before, during, and after medical training is important. Equally important is picking the right partner - they're the one family member you get to choose.
Overall, Dr Gebien's story serves as an excellent case study in the hazards of being a physician, and the failings too many of us assume we'll avoid just by having an MD after our names. He doesn't come across well in telling his own story, and there are numerous areas to find fault in beyond just his addiction. Yet, that makes his story all the more valuable to share. Being a doctor doesn't make anyone special, better, or more capable at handling the challenges of life. When physicians start to think that it does, they start engaging in behaviours that are destructive to their own lives or, as Dr Gebien's story briefly mentions, the lives of loved ones and colleagues. Staying grounded, staying humble, and remaining self-critical of our own behaviours is critical for physicians.
Wanted to touch on a story that's rightfully making the rounds on social media, of a Canadian physician talking about his addiction to Fentanyl. Fentanyl is the new addict drug of choice in much of Canada, particularly in southern Ontario. It's been building for a few years. Every conversation I have with those in addictions or drug enforcement says that this is where we're seeing a big focus. It's a very powerful narcotic, one that's definitely overprescribed, and it has numerous routes of absorption. In many ways, it's the most recent culmination of the wider opioid crisis that's been growing for decades now.
Dr Gebien's tale is worth reading for its account of the devastating effects of opioid addiction, and the hubris of physicians who think they're immune to such common human failings. On the former point, there's enough written by more knowledgeable people than me that I won't say much besides a reiteration that I want my practice to be very opioid-averse. As far as I'm concerned, unless something's going to cure your pain very soon (usually by an operation of some sort), or we expect you to die at some point in the near future, I have trouble seeing the role of opioids. They don't work well long term, they're addictive, and they come with tons of side-effects. They're not really a treatment for pain, they're a way to stall it in the short-term.
On the second point, it can't be emphasized enough - doctors are human and we fall victim to all the things humans fall victim to, including addiction. One particular point to mention about this story is the hazards of self-prescribing. Physicians are not supposed to treat anyone who isn't their patient, including themselves. That means no treating family or friends except in very unique circumstances. That means no treating co-workers. That means no treating fellow physicians unless they're in your office for a valid reason. I can't say how often I've seen a physician write off a prescription to one of their colleagues based on that colleague's word alone. No history. No physical. No investigations. Just "I need this script, can you help me out?", and bam, done. In one instance, a physician asked a colleague for a medication for their child, effectively treating their own kid with the help of a fellow physician who never even laid eyes on that child! Don't do this. Yes, it sucks to have to go to your GP to get a simple script. Yes, you know exactly what needs to be done. You know who else it sucks for to have to do that? EVERYONE! Being a physician should not get you a fast track to basic medical care, nor should it allow you to skip the basic components of treatment, such as a proper evaluation. Please, colleagues, supervisors, and anyone coming afterwards, just don't do this, and don't help others do this. It's unethical and can lead to some very dark outcomes.
There's a few other elements to this story that deserve a quick mention, since they probably contributed to his situation and are much more common traps for physicians to fall into then addiction. First is proper money management. He was making $300k a year and needed parental assistance to cover two rehab-related bills of $10k and $80k, in addition to needing to put $35k on a line-of-credit. Everyone, regardless of profession, should have an Emergency fund of at least 6 months of living expenses, ideally 1 year's worth. In his case, it doesn't sound like he had anywhere close to that. I don't doubt that a fair bit of money was going to feed or hide is addiction. Yet, there are other clear missteps. Buying a large house, luxury cars, and a boat weren't necessary and probably weren't affordable. Even if your means are great, you still need to live within them.
Secondly, this story highlights the need for a robust support system. Here we see only one side of the story, so it's hard to draw conclusions, but I don't get the sense of a reliable base of support from Dr Gebien's wife or parents. Their relationships seem dysfunctional and his mother, who looked to be dealing with her own problems of opioid use, was an enabler in his addiction. Building connections with reliable people before, during, and after medical training is important. Equally important is picking the right partner - they're the one family member you get to choose.
Overall, Dr Gebien's story serves as an excellent case study in the hazards of being a physician, and the failings too many of us assume we'll avoid just by having an MD after our names. He doesn't come across well in telling his own story, and there are numerous areas to find fault in beyond just his addiction. Yet, that makes his story all the more valuable to share. Being a doctor doesn't make anyone special, better, or more capable at handling the challenges of life. When physicians start to think that it does, they start engaging in behaviours that are destructive to their own lives or, as Dr Gebien's story briefly mentions, the lives of loved ones and colleagues. Staying grounded, staying humble, and remaining self-critical of our own behaviours is critical for physicians.
Saturday, 4 March 2017
Comments on the Match
With the match now over and my class now aware of their results, we've had a bit of time to decompress and look ahead to residency preparations. On that latter point, there is a lot to get done - forms to fill out, organizations to sign-up with, some certifications to arrange, figuring out how to get paid (but yay, money!).
While I know where most of my class is headed now, it's all been through voluntary disclosures, which means I pretty much only know about my classmates who are happy with their results (and all the classmates I'm closer to all matched). Seems like my school had a pretty good year, but I know I'm only getting a partial picture. We do get a debrief on the school's overall match results soon, so I'll know more then. Here's hoping my class did as well as I think they did, and those who didn't match are getting enough support for the next steps.
I wanted to comment quickly on the only match stats we have at this time - the list of spots left unfilled from the 1st iteration. Interpretation of these is always a bit hazardous, as these positions mix both the CMG and IMG unfilled positions together. You can make some inferences, but there's naturally a bit of guesswork.
Some of the results aren't terribly surprising. There's a handful of positions left in the smaller, more technical fields with poorer job prospects. There's a few positions in typically competitive fields (like Derm) that are most likely IMG spots that were intentionally left unfilled. And there's the crush of positions in Quebec that go habitually unfilled as Quebec oversupplies its residency positions.
Some of the results aren't exactly shocking, but are notable. Internal filled almost every spot. Internal did see a jump in competitiveness last year, and the word is that trend continued in a big way this year. While this data doesn't confirm that perception on its own, it's certainly consistent with it. In the other direction, Psychiatry had a few more unfilled spots than I expected, given that it is also garnering a bit more attention. Psychiatry has been steadily gaining positions, however, and the remaining spots are generally in more remote locations - ironically, the places that are probably lacking the psychiatrists those extra positions were meant to train.
Lastly, Family Medicine had an absolute ton of unfilled spots this year. Family usually has a number, but the proportion of Family spots left open is greater than it has been in the recent past. Interest in Family, which took a bit of a dip last year, may be a bit low this year as well. That would fit with the notion that Internal has jumped in popularity - while overall competitiveness for CMGs in CaRMS has increased somewhat, Internal is a huge specialty and for it to become more competitive means other larger specialties have to get less competitive. It makes sense that a rise in interest in Internal would be coupled with a drop in interest in Family. We'll have to see when the full match stats eventually come out.
While I know where most of my class is headed now, it's all been through voluntary disclosures, which means I pretty much only know about my classmates who are happy with their results (and all the classmates I'm closer to all matched). Seems like my school had a pretty good year, but I know I'm only getting a partial picture. We do get a debrief on the school's overall match results soon, so I'll know more then. Here's hoping my class did as well as I think they did, and those who didn't match are getting enough support for the next steps.
I wanted to comment quickly on the only match stats we have at this time - the list of spots left unfilled from the 1st iteration. Interpretation of these is always a bit hazardous, as these positions mix both the CMG and IMG unfilled positions together. You can make some inferences, but there's naturally a bit of guesswork.
Some of the results aren't terribly surprising. There's a handful of positions left in the smaller, more technical fields with poorer job prospects. There's a few positions in typically competitive fields (like Derm) that are most likely IMG spots that were intentionally left unfilled. And there's the crush of positions in Quebec that go habitually unfilled as Quebec oversupplies its residency positions.
Some of the results aren't exactly shocking, but are notable. Internal filled almost every spot. Internal did see a jump in competitiveness last year, and the word is that trend continued in a big way this year. While this data doesn't confirm that perception on its own, it's certainly consistent with it. In the other direction, Psychiatry had a few more unfilled spots than I expected, given that it is also garnering a bit more attention. Psychiatry has been steadily gaining positions, however, and the remaining spots are generally in more remote locations - ironically, the places that are probably lacking the psychiatrists those extra positions were meant to train.
Lastly, Family Medicine had an absolute ton of unfilled spots this year. Family usually has a number, but the proportion of Family spots left open is greater than it has been in the recent past. Interest in Family, which took a bit of a dip last year, may be a bit low this year as well. That would fit with the notion that Internal has jumped in popularity - while overall competitiveness for CMGs in CaRMS has increased somewhat, Internal is a huge specialty and for it to become more competitive means other larger specialties have to get less competitive. It makes sense that a rise in interest in Internal would be coupled with a drop in interest in Family. We'll have to see when the full match stats eventually come out.
Wednesday, 1 March 2017
Matched
Quick update because I'm still processing the result - successfully matched today in Family Medicine to my top-choice program. Whew.
It's a huge sigh of relief, but I know it means that the real work is only just beginning. I now have a ticking clock of two short years to get myself practice-ready. It all feels very real now, but I'm pretty excited knowing that this is where the stakes get higher. Onwards and upwards and all that!
It's a huge sigh of relief, but I know it means that the real work is only just beginning. I now have a ticking clock of two short years to get myself practice-ready. It all feels very real now, but I'm pretty excited knowing that this is where the stakes get higher. Onwards and upwards and all that!
Tuesday, 28 February 2017
Match Day - Tomorrow
Ugh...
Argh...
Ahhh...
So, tomorrow's match day. I've been trying to distract myself from that fact for well over a week now and my level success is pretty low at this stage. At noon, I find out my fate moving forward. So does the rest of my class. For the record, communal anxiety is not helpful for personal anxiety!
My school has done the only thing that makes sense to me and gives us the whole day off. I think I could have tolerated morning classes, but having the afternoon off is a huge relief. Whether I'm happy, sad, or just confused, I'll have the time to handle it on my own terms, rather than have to deal with a bunch of lectures, tasks, or people I'd rather just avoid. Apparently years ago they used to hand out sealed envelopes to everyone in the same room and you were supposed to open them together. That sounds mortifying.
In any case, thumbs up to the home school for doing the right thing. Here's hoping I get to use that time to celebrate.
Argh...
Ahhh...
So, tomorrow's match day. I've been trying to distract myself from that fact for well over a week now and my level success is pretty low at this stage. At noon, I find out my fate moving forward. So does the rest of my class. For the record, communal anxiety is not helpful for personal anxiety!
My school has done the only thing that makes sense to me and gives us the whole day off. I think I could have tolerated morning classes, but having the afternoon off is a huge relief. Whether I'm happy, sad, or just confused, I'll have the time to handle it on my own terms, rather than have to deal with a bunch of lectures, tasks, or people I'd rather just avoid. Apparently years ago they used to hand out sealed envelopes to everyone in the same room and you were supposed to open them together. That sounds mortifying.
In any case, thumbs up to the home school for doing the right thing. Here's hoping I get to use that time to celebrate.
Saturday, 25 February 2017
Considering a Career in Medicine - SCIENCE!
We focus a lot on how students can prove they're good enough for medicine. These posts are for students wondering if medicine is good enough for them.
Short Version: Medicine absolutely requires a solid understanding of scientific principles and facts, as well as an ability to critically analyze new scientific studies or discoveries. The common undergraduate precursors to a career in medicine are based in scientific study, for good reason. Scientific research is intimately connected to medicine, and involvement in research can be beneficial to a prospective physicians' career goals before, during, and after medical school. An interest in science is therefore a common reason why students choose to pursue medicine.
Medicine is an inherently applied field, however - when it comes to the nuts and bolts of scientific discovery, the basic or fundamental research that underlies much of humanity's technological progress, physicians rarely get involved. Rather, physicians involved in research tend to spend most of their time on clinical research, which investigates potential applications of discoveries others have made. This can be an advantage or a disadvantage, depending on individual preferences. Science-loving potential medical students should give some thought to how they want to incorporate scientific knowledge into their careers and ensure that being a physician will satisfy that objective.
Long Version: Modern medicine could not exist without the development of the scientific method and its continual application to new realms of human knowledge. To the extent physicians' interventions are effective in preventing death or improving life, it is thanks to the works of physicians and scientists in the past and present. As such, it is impossible for a capable physician to exist without a solid understanding of both prior scientific discoveries as well as the process that leads to new scientific discoveries.
Furthermore, the pathway to become a physician, with some uncommon exceptions, requires a solid scientific background. Medical school admissions has moved away from requiring certain degrees or pre-requisite courses, but most still require the science-heavy MCAT and the vast majority of medical students do their undergraduate education in science, math, social sciences, or engineering. Put simply, the pathway to medicine runs through science and therefore medicine attracts those with a proclivity towards scientific study.
Part of the path to medicine for many students includes becoming actively involved in scientific research. Research is by no means required for admissions to any medical school in Canada, but it can certainly help with the admissions process at the majority of schools. Even at schools that do not consider research in their admissions process, or do not weigh it heavily, many matriculants will have significant research experience. There continues to be some value to engaging in research after admissions. Many residency programs will take research experience into account. This is usually as a secondary consideration to clinical performance, however, and research is really only required for a few highly-competitive fields. Once in residency, most programs will have required research projects, and research productivity can be important for landing positions after residency, depending on specialty and desired location of employment.
Yet, despite its close ties to the study and advancement of scientific knowledge, medicine is far more concerned with application of new discoveries than in their production. Physicians are largely involved with what is termed "clinical research" as opposed to foundational research or basic sciences research. To oversimplify somewhat, clinical research involves study on humans. For ethical reasons, we tend not to allow such research without having some expectation as to what will happen, so clinical research generally involves relying heavily on knowledge derived from basic sciences research, typically performed by non-physicians. This is not to diminish the difficulty or importance of clinical research, which is fraught with challenges and is critical to developing truly evidence-based medical practice. However, it does speak to the place of physicians within the process of developing new approaches to medicine - if a useful new intervention in medicine takes 100 steps to become discovered, developed, optimized, and proven effective, physicians involved in research are usually responsible for the last couple steps only, with an emphasis on optimization and proving efficacy rather than on discovery or development.
To many, this limited role of physicians in the scientific process is not a drawback. Many physicians have no desire to be involved in research at all, even those enthralled by the miracles of science. Medicine is vast and learning how properly apply the ocean of scientific information relevant to one's practice can be plenty of mental stimulation for science-minded individuals. Similarly, for those interested in advancing medical knowledge but are uninterested in the basic sciences research students typically encounter in their undergraduate studies, clinical research can be an ideal way to satisfy that objective.
At this point, the growing demographic of clinician-scientists deserves recognition. Clinician-scientists are physicians who have additional training towards becoming capable researchers, usually through intensive graduate work. In some cases, the focus remains on clinical research, with clinician-scientists doing much the same research that an academic physician without additional training would undertake, but with perhaps a bit more expertise and often with a greater proportion of time spent on research activities rather than on clinical duties. Other clinician-scientists, however, will try to straddle the divide between clinical and basic sciences research. Translational research, with its emphasis on taking or making new scientific discoveries and bringing them into clinical practice, is receiving substantial attention in academic circles. Clinician-scientists, with focused training in basic sciences research, are considered ideally placed to take advantage of these opportunities.
The number of these clinician-scientists is fairly small, however, and not without reason. Becoming established as both a clinician and basic sciences researcher requires a substantial amount of time. A physician typically does not enter independent practice until their early 30's, and the same can be said for most basic sciences researchers. To manage a career in both areas can easily require a person to train into their late 30's or early 40's before independence in medical practice and research are achieved. That additional time spent training means losing significant financial opportunities, that extended training delays entry into employment. Additionally, research tends to pay less than clinical work, meaning clinician-scientists often earn less than their clinician-only counterparts.
Additionally, not all who pursue clinician-scientist training take advantage of both their intended roles. Many individuals who obtain both an MD and a PhD, whether that PhD was obtained before, during, or after medical school, do no research or research that could easily be accomplished with an MD alone. Likewise, there is a small group of clinician-scientists who no longer work with patients in a clinical setting, or who have minimal clinical duties, effectively working off their PhD alone. Obtaining both an MD and PhD can be an attractive prospect for highly ambitious students, but should be approached with caution and with as full an understanding of the clinician-scientist role as possible.
To summarize, medicine absolute involves scientific knowledge and benefits from those interested in science. Being interested in science is a good reason to consider medicine! Yet, potential medical students must keep in mind that an MD prepares students to be clinicians first and researchers second, with a focus on clinical research only. A physician's use of scientific knowledge is usually confined to direct applications for patients. For those who would strongly prefer to do research outside of a clinical setting, or those who have minimal interest in working with patients, an MD may not be the best fit, and those students would likely be better served in a PhD-only program. For those who truly want to do both, the clinician-scientist route, which usually involves completion of both an MD and a PhD, may be worthwhile. Science-lovers should take the time to check out all their options before diving into a career in medicine that may or may not be tailored to their specific interests.
Short Version: Medicine absolutely requires a solid understanding of scientific principles and facts, as well as an ability to critically analyze new scientific studies or discoveries. The common undergraduate precursors to a career in medicine are based in scientific study, for good reason. Scientific research is intimately connected to medicine, and involvement in research can be beneficial to a prospective physicians' career goals before, during, and after medical school. An interest in science is therefore a common reason why students choose to pursue medicine.
Medicine is an inherently applied field, however - when it comes to the nuts and bolts of scientific discovery, the basic or fundamental research that underlies much of humanity's technological progress, physicians rarely get involved. Rather, physicians involved in research tend to spend most of their time on clinical research, which investigates potential applications of discoveries others have made. This can be an advantage or a disadvantage, depending on individual preferences. Science-loving potential medical students should give some thought to how they want to incorporate scientific knowledge into their careers and ensure that being a physician will satisfy that objective.
Long Version: Modern medicine could not exist without the development of the scientific method and its continual application to new realms of human knowledge. To the extent physicians' interventions are effective in preventing death or improving life, it is thanks to the works of physicians and scientists in the past and present. As such, it is impossible for a capable physician to exist without a solid understanding of both prior scientific discoveries as well as the process that leads to new scientific discoveries.
Furthermore, the pathway to become a physician, with some uncommon exceptions, requires a solid scientific background. Medical school admissions has moved away from requiring certain degrees or pre-requisite courses, but most still require the science-heavy MCAT and the vast majority of medical students do their undergraduate education in science, math, social sciences, or engineering. Put simply, the pathway to medicine runs through science and therefore medicine attracts those with a proclivity towards scientific study.
Part of the path to medicine for many students includes becoming actively involved in scientific research. Research is by no means required for admissions to any medical school in Canada, but it can certainly help with the admissions process at the majority of schools. Even at schools that do not consider research in their admissions process, or do not weigh it heavily, many matriculants will have significant research experience. There continues to be some value to engaging in research after admissions. Many residency programs will take research experience into account. This is usually as a secondary consideration to clinical performance, however, and research is really only required for a few highly-competitive fields. Once in residency, most programs will have required research projects, and research productivity can be important for landing positions after residency, depending on specialty and desired location of employment.
Yet, despite its close ties to the study and advancement of scientific knowledge, medicine is far more concerned with application of new discoveries than in their production. Physicians are largely involved with what is termed "clinical research" as opposed to foundational research or basic sciences research. To oversimplify somewhat, clinical research involves study on humans. For ethical reasons, we tend not to allow such research without having some expectation as to what will happen, so clinical research generally involves relying heavily on knowledge derived from basic sciences research, typically performed by non-physicians. This is not to diminish the difficulty or importance of clinical research, which is fraught with challenges and is critical to developing truly evidence-based medical practice. However, it does speak to the place of physicians within the process of developing new approaches to medicine - if a useful new intervention in medicine takes 100 steps to become discovered, developed, optimized, and proven effective, physicians involved in research are usually responsible for the last couple steps only, with an emphasis on optimization and proving efficacy rather than on discovery or development.
To many, this limited role of physicians in the scientific process is not a drawback. Many physicians have no desire to be involved in research at all, even those enthralled by the miracles of science. Medicine is vast and learning how properly apply the ocean of scientific information relevant to one's practice can be plenty of mental stimulation for science-minded individuals. Similarly, for those interested in advancing medical knowledge but are uninterested in the basic sciences research students typically encounter in their undergraduate studies, clinical research can be an ideal way to satisfy that objective.
At this point, the growing demographic of clinician-scientists deserves recognition. Clinician-scientists are physicians who have additional training towards becoming capable researchers, usually through intensive graduate work. In some cases, the focus remains on clinical research, with clinician-scientists doing much the same research that an academic physician without additional training would undertake, but with perhaps a bit more expertise and often with a greater proportion of time spent on research activities rather than on clinical duties. Other clinician-scientists, however, will try to straddle the divide between clinical and basic sciences research. Translational research, with its emphasis on taking or making new scientific discoveries and bringing them into clinical practice, is receiving substantial attention in academic circles. Clinician-scientists, with focused training in basic sciences research, are considered ideally placed to take advantage of these opportunities.
The number of these clinician-scientists is fairly small, however, and not without reason. Becoming established as both a clinician and basic sciences researcher requires a substantial amount of time. A physician typically does not enter independent practice until their early 30's, and the same can be said for most basic sciences researchers. To manage a career in both areas can easily require a person to train into their late 30's or early 40's before independence in medical practice and research are achieved. That additional time spent training means losing significant financial opportunities, that extended training delays entry into employment. Additionally, research tends to pay less than clinical work, meaning clinician-scientists often earn less than their clinician-only counterparts.
Additionally, not all who pursue clinician-scientist training take advantage of both their intended roles. Many individuals who obtain both an MD and a PhD, whether that PhD was obtained before, during, or after medical school, do no research or research that could easily be accomplished with an MD alone. Likewise, there is a small group of clinician-scientists who no longer work with patients in a clinical setting, or who have minimal clinical duties, effectively working off their PhD alone. Obtaining both an MD and PhD can be an attractive prospect for highly ambitious students, but should be approached with caution and with as full an understanding of the clinician-scientist role as possible.
To summarize, medicine absolute involves scientific knowledge and benefits from those interested in science. Being interested in science is a good reason to consider medicine! Yet, potential medical students must keep in mind that an MD prepares students to be clinicians first and researchers second, with a focus on clinical research only. A physician's use of scientific knowledge is usually confined to direct applications for patients. For those who would strongly prefer to do research outside of a clinical setting, or those who have minimal interest in working with patients, an MD may not be the best fit, and those students would likely be better served in a PhD-only program. For those who truly want to do both, the clinician-scientist route, which usually involves completion of both an MD and a PhD, may be worthwhile. Science-lovers should take the time to check out all their options before diving into a career in medicine that may or may not be tailored to their specific interests.
Saturday, 18 February 2017
Pets and Private Health Care
About a week ago, my dog had an unfortunately run-in with another dog - who we know and is usually friendly - that resulted in him getting nipped pretty hard in his side. Wasn't too bad, but deep enough that it couldn't be left to heal on its own, particularly as the other dog had been carrying around a dead carcass of something or other in its mouth just prior (hence the nip, as my dog got interested and the other dog got defensive about their new prize).
It was late at night when we noticed the injury, so we took him to the emergency veterinary clinic to avoid letting him sit with it overnight. We were hoping for a quick clean-out and stitch, but because our dog is giant, easily frightened, and we couldn't rule out a bad contamination from the bite, the vet quite reasonably want to explore the wound under light sedation. We were given a quote before going ahead with anything and the final bill lined up with that quote perfectly, about $500.
In short, it was professional, competent care with excellent price transparency.
And yet, I'm in a very fortunate position to be able to afford that $500 of care. Many people couldn't, especially for a pet. If I was in a worse economic situation, I could have had to gamble that my dog would heal on his own. With his small wound, he would likely have done just fine, but it would still involve an element of risk for his well-being.
Why do I bring this up? Well, because private healthcare is back in the mix in Canada.
Now, "private healthcare" is about as vague a term as you can get. Canadian health services are largely provided by private organizations, just funded from mostly public sources. Yet most people wouldn't call Canadian healthcare private. Likewise, when discussing current efforts to allow private billing of provincially-insured healthcare services, there are a multitude of schemes that could be considered. Furthermore, when the Canadian healthcare system gets compared to other countries' systems with private components, it often gets forgotten that those countries actually have more government funding as a proportion of medical expenses than Canada does.
Therefore, when I speak of the encroachment of private healthcare in Canada, it's hard to do so without oversimplifying the debate, and I want to acknowledge that before going any further on this point.
Currently, there are more than a few physician groups and individual physicians expressing support for allowing private billing for otherwise publicly-covered healthcare services. In some cases, physicians have already opened such clinics and are operating them with questionable legality. One BC lawsuit is currently underway concerning such a clinic, this one focused on outpatient surgeries. In my experience thus far, a desire for a private option, or at least a belief that it is necessary, helpful, or inevitable, is a popular opinion among physicians. The notion is that private care could cover something lacking in our current public system, even if it's as simple as providing additional capacity for elective procedures.
My objection is that no matter the formulation, unless we dramatically reshape the public system as well, private care will provide some services of consequence to outcomes to some who can pay, but not to others who cannot. The only alternative is if private care adds no value whatsoever, in which case, what's the point? I felt enough worry about having to cover the costs for care of my dog with a condition that was relatively safe, with expenses I could afford, and when everything about his care went perfectly. To have to make that decision with a higher cost, a more serious condition, and the real possibility of sub-optimal outcomes would be so much worse. To make that decision for a human - myself or another loved one - would be even more difficult, as much as I love my dog. I also never want to be on the other side of this situation, having to ask patients to choose between their physical and financial health. For pets and other animals, these sorts of decisions are unavoidable - I don't think we'll ever have universal veterinary care. Yet, we can avoid these decisions for people, if we maintain and strengthen the public system we have now.
For the record, my dog is now fine. His wound is healing well with no signs of infection. He was a little anxious for the first day or two and is pretty upset that he has to wear a cone, but he's more or less back to his old, affectionate self!
It was late at night when we noticed the injury, so we took him to the emergency veterinary clinic to avoid letting him sit with it overnight. We were hoping for a quick clean-out and stitch, but because our dog is giant, easily frightened, and we couldn't rule out a bad contamination from the bite, the vet quite reasonably want to explore the wound under light sedation. We were given a quote before going ahead with anything and the final bill lined up with that quote perfectly, about $500.
In short, it was professional, competent care with excellent price transparency.
And yet, I'm in a very fortunate position to be able to afford that $500 of care. Many people couldn't, especially for a pet. If I was in a worse economic situation, I could have had to gamble that my dog would heal on his own. With his small wound, he would likely have done just fine, but it would still involve an element of risk for his well-being.
Why do I bring this up? Well, because private healthcare is back in the mix in Canada.
Now, "private healthcare" is about as vague a term as you can get. Canadian health services are largely provided by private organizations, just funded from mostly public sources. Yet most people wouldn't call Canadian healthcare private. Likewise, when discussing current efforts to allow private billing of provincially-insured healthcare services, there are a multitude of schemes that could be considered. Furthermore, when the Canadian healthcare system gets compared to other countries' systems with private components, it often gets forgotten that those countries actually have more government funding as a proportion of medical expenses than Canada does.
Therefore, when I speak of the encroachment of private healthcare in Canada, it's hard to do so without oversimplifying the debate, and I want to acknowledge that before going any further on this point.
Currently, there are more than a few physician groups and individual physicians expressing support for allowing private billing for otherwise publicly-covered healthcare services. In some cases, physicians have already opened such clinics and are operating them with questionable legality. One BC lawsuit is currently underway concerning such a clinic, this one focused on outpatient surgeries. In my experience thus far, a desire for a private option, or at least a belief that it is necessary, helpful, or inevitable, is a popular opinion among physicians. The notion is that private care could cover something lacking in our current public system, even if it's as simple as providing additional capacity for elective procedures.
My objection is that no matter the formulation, unless we dramatically reshape the public system as well, private care will provide some services of consequence to outcomes to some who can pay, but not to others who cannot. The only alternative is if private care adds no value whatsoever, in which case, what's the point? I felt enough worry about having to cover the costs for care of my dog with a condition that was relatively safe, with expenses I could afford, and when everything about his care went perfectly. To have to make that decision with a higher cost, a more serious condition, and the real possibility of sub-optimal outcomes would be so much worse. To make that decision for a human - myself or another loved one - would be even more difficult, as much as I love my dog. I also never want to be on the other side of this situation, having to ask patients to choose between their physical and financial health. For pets and other animals, these sorts of decisions are unavoidable - I don't think we'll ever have universal veterinary care. Yet, we can avoid these decisions for people, if we maintain and strengthen the public system we have now.
For the record, my dog is now fine. His wound is healing well with no signs of infection. He was a little anxious for the first day or two and is pretty upset that he has to wear a cone, but he's more or less back to his old, affectionate self!
Tuesday, 14 February 2017
Research and Other Extra-Curriculars
My medical school experience has been characterized by a decent amount of research and a LOT of extra-curriculars. Medical students in general are fairly active people, usually very eager to take on that one extra task, though at some point towards the end of second year or beginning of third year, I realized I had taken on just a little too much. Too many projects on the go and in the rush of clerkship, nowhere near enough time to do them all well.
So, about half-way through clerkship, I started pulling back. I left a few minor projects to fall by the wayside, delayed a few others or worked on them slowly, and wrapped up the ones I could. This helped me get through clerkship without losing my mind to stress, and I still managed to come away with what I think is a reasonable list of accomplishments through my previous 3+ years.
Yet, on one of my electives, I had a preceptor who embodied the concept of going above and beyond as a complete physician. Involved in both social and academic endeavours, he seem as enthralled by the non-clinical aspects of his work as he was by his clinical duties. You could tell that his enthusiasm for one area helped maintain his enthusiasm overall, in addition to keeping him at the forefront of knowledge. Granted, I had some reservations about some of his ideas, as his eagerness for their benefit didn't always match available evidence in my mind, but I can't help but admire that enduring passion.
Now that I'm back in class, with a lighter schedule and ample time to pursue some outside interests, it's been very tempting to stick with a low workload in terms of extra-curriculars. Yet, I pursued those extra-curriculars in the first place because I enjoyed them, because they made medicine itself more fulfilling and meaningful. My elective preceptor seemed to be of the same mindset, that the variety and diversity of projects - even though challenging - helped make medicine enjoyable. So, I've jumped back into a few. Just a few, and mostly at arms' length. I don't have the time to get much deeper into things, with (hopefully) only a few months left in my training. It's a nice balance at the moment.
Residency will put that balancing act to the test. For personal and professional reasons, I would like to be a bit more involved in non-clinical aspects than I was in clerkship. I'm counting on the fact that I'll be more familiar with the whole system and will generally have more stability in my rotations to help facilitate that, but weighed against the added responsibilities and pressures of residency, I'm likely being overly optimistic. Nevertheless, I think having a foot in the different aspects relevant to medicine is worthwhile.
While I do believe medicine should focus on a small set of core competencies, without the implication that physicians should be anything and everything, the advantage of being a true professional is the ability to branch out to satisfy interests and community needs. My elective time with this particular preceptor was a good reminder that this diversity was a major driver for me to enter medicine in the first place.
So, about half-way through clerkship, I started pulling back. I left a few minor projects to fall by the wayside, delayed a few others or worked on them slowly, and wrapped up the ones I could. This helped me get through clerkship without losing my mind to stress, and I still managed to come away with what I think is a reasonable list of accomplishments through my previous 3+ years.
Yet, on one of my electives, I had a preceptor who embodied the concept of going above and beyond as a complete physician. Involved in both social and academic endeavours, he seem as enthralled by the non-clinical aspects of his work as he was by his clinical duties. You could tell that his enthusiasm for one area helped maintain his enthusiasm overall, in addition to keeping him at the forefront of knowledge. Granted, I had some reservations about some of his ideas, as his eagerness for their benefit didn't always match available evidence in my mind, but I can't help but admire that enduring passion.
Now that I'm back in class, with a lighter schedule and ample time to pursue some outside interests, it's been very tempting to stick with a low workload in terms of extra-curriculars. Yet, I pursued those extra-curriculars in the first place because I enjoyed them, because they made medicine itself more fulfilling and meaningful. My elective preceptor seemed to be of the same mindset, that the variety and diversity of projects - even though challenging - helped make medicine enjoyable. So, I've jumped back into a few. Just a few, and mostly at arms' length. I don't have the time to get much deeper into things, with (hopefully) only a few months left in my training. It's a nice balance at the moment.
Residency will put that balancing act to the test. For personal and professional reasons, I would like to be a bit more involved in non-clinical aspects than I was in clerkship. I'm counting on the fact that I'll be more familiar with the whole system and will generally have more stability in my rotations to help facilitate that, but weighed against the added responsibilities and pressures of residency, I'm likely being overly optimistic. Nevertheless, I think having a foot in the different aspects relevant to medicine is worthwhile.
While I do believe medicine should focus on a small set of core competencies, without the implication that physicians should be anything and everything, the advantage of being a true professional is the ability to branch out to satisfy interests and community needs. My elective time with this particular preceptor was a good reminder that this diversity was a major driver for me to enter medicine in the first place.
Tuesday, 7 February 2017
What's in the Scope of Medicine?
Physicians are privileged among healthcare practitioners in that medicine's scope, both functionally and legally, is essentially unbounded from a professional standpoint. While other healthcare professions are limited somewhat in what's considered their area of expertise, particularly from a legal perspective, physicians generally are not, with some obvious exceptions (dental work, for example).
Unfortunately, this also leaves unbounded the amount of information or expertise that could be considered worthwhile for a physician to learn. Any medical student past their first semester will have experienced this, sitting through more than a few lectures where some emphasized pieces of information appear to be relevant to the eventual practice of maybe 1% of the class only. Even as a future generalist, I can think of quite a bit that I've learned over the past 4 years that I will likely never have to use in clinical practice, even if some of my classmates will.
Physicians are also starting to explore areas outside of what is typically considered clinical medicine. For example, as the profession rightly acknowledges the high impact of social factors on health, medicine is slowly expanding to include, well, virtually anything. Everything from urban infrastructure, to primary education, to environmental regulations, to immigration, to energy policy touches on human health in significant ways. We have some teaching about these factors in medical school, but not overly in-depth, nor do we have time to touch on everything in society conceivably impacting health.
While I love learning about these "other" parts of healthcare outside of standard clinical medicine and finding ways to incorporate them into practice, it's unrealistic to expect me or anyone else to be masters of even a fraction of this material. This begs the question - what is essential for all physicians to know, and what is not? I don't believe we have answered this question particularly well and I believe it needs a good answer.
Physicians are fortunate to be able to push or around through the barriers that constrain other healthcare professionals from doing novel work outside their scope, because our scope is so ill-defined, and it leads to a lot of innovation within our healthcare system. That ability to innovate is worth preserving. The downside is that as we allow physicians to be just about anything these days, we've started structuring our medical education system to push physicians to be everything. This is neither realistic nor optimal.
At some point, we need to introduce more flexibility into our medical education to match the flexibility we expect from our practicing physicians. That means developing a core base of competency that is relevant to virtually everyone at that stage of training which is emphasized heavily, but then making much of what we currently teach non-mandatory. To compensate, more selective, elective, and extra-curricular education should be incorporated. Admittedly, this takes a degree of coordination medical schools and residency programs have not proven to be too adept at handling in the past. However, as medicine grows ever-wider, medical educators will have to start recognizing the limits of what can be taught and start seriously considering what should be taught, even if that means eliminating useful elements from what is currently part of the mandatory curriculum.
Unfortunately, this also leaves unbounded the amount of information or expertise that could be considered worthwhile for a physician to learn. Any medical student past their first semester will have experienced this, sitting through more than a few lectures where some emphasized pieces of information appear to be relevant to the eventual practice of maybe 1% of the class only. Even as a future generalist, I can think of quite a bit that I've learned over the past 4 years that I will likely never have to use in clinical practice, even if some of my classmates will.
Physicians are also starting to explore areas outside of what is typically considered clinical medicine. For example, as the profession rightly acknowledges the high impact of social factors on health, medicine is slowly expanding to include, well, virtually anything. Everything from urban infrastructure, to primary education, to environmental regulations, to immigration, to energy policy touches on human health in significant ways. We have some teaching about these factors in medical school, but not overly in-depth, nor do we have time to touch on everything in society conceivably impacting health.
While I love learning about these "other" parts of healthcare outside of standard clinical medicine and finding ways to incorporate them into practice, it's unrealistic to expect me or anyone else to be masters of even a fraction of this material. This begs the question - what is essential for all physicians to know, and what is not? I don't believe we have answered this question particularly well and I believe it needs a good answer.
Physicians are fortunate to be able to push or around through the barriers that constrain other healthcare professionals from doing novel work outside their scope, because our scope is so ill-defined, and it leads to a lot of innovation within our healthcare system. That ability to innovate is worth preserving. The downside is that as we allow physicians to be just about anything these days, we've started structuring our medical education system to push physicians to be everything. This is neither realistic nor optimal.
At some point, we need to introduce more flexibility into our medical education to match the flexibility we expect from our practicing physicians. That means developing a core base of competency that is relevant to virtually everyone at that stage of training which is emphasized heavily, but then making much of what we currently teach non-mandatory. To compensate, more selective, elective, and extra-curricular education should be incorporated. Admittedly, this takes a degree of coordination medical schools and residency programs have not proven to be too adept at handling in the past. However, as medicine grows ever-wider, medical educators will have to start recognizing the limits of what can be taught and start seriously considering what should be taught, even if that means eliminating useful elements from what is currently part of the mandatory curriculum.
Subscribe to:
Posts (Atom)