I've decided to write the USMLE Step 1 towards the end of this summer for two reasons.
1) US fellowships. There's a small chance I'll wind up doing a fellowship in the US and having the USMLE already written can be helpful for some of those US fellowships.
It's all very up-in-the-air at this point - I'm not considering too many fellowship-heavy specialties that would be greatly helped by a high-quality US fellowship, but I also love some of the more academic parts of medicine like research or teaching where a fellowship may be more useful. It'll be years before that gets figured out, obviously, but if I do go the super-intense fellowship route, it'll be worthwhile to have options in the US. All I need is a pass, so the bar isn't super high.
2) Clerkship prep. There's a lot of pre-clerkship information that's useful for clerkship that I've already forgotten, never learned, or never even been introduced to. Studying for the USMLE is forcing me to go over much of that information.
It also better fits my studying style than what I've experienced in pre-clerkship, where it feels like there's a lot of short-term memorization. When your major test on a subject comes only a few weeks after you start learning about that subject, there's not much time to really let information bounce around in your head. You have to learn it and be ready to spit it out again quickly. Then, since the only subsequent reason to revisit that information comes at most a few months later for and end-of-semester test, that information can get lost quickly, especially as new subjects pop up to demand your mental resources.
This sort of all-encompassing "big test" studying fits my preferred learning style well. I'll have to go over a subject and learn it as best I can, but it'll have to fit in with all the other subjects also on the test. That requires some periodic efforts to go back to material I had already studied, to make sure it's still in my brain.
I hope this strategy'll work - and that it'll pay off in clerkship, when I'll want to impress with my knowledge base (or at least not look like an idiot). I guess I'll find out soon enough!
Sunday, 29 March 2015
Extraocular Muscles
We're in the midst of a short session learning about the eye. For the most part it's fairly interesting and understandable, but I'm beating my head against the wall trying to understand extraocular muscles' functions. The four straight ones (the rectus mucles) are pretty obvious, but the oblique ones are horribly confusing. I've found about half a dozen different sources each telling me a they have a different function.
I think I know which sources are right - and even why the other sources say what they do (mostly a confusion between the function of the muscles, what happens when they're damaged, and how to test them), but wow, that was a lot of searching to get a relatively simple answer.
Friday, 27 March 2015
Single Slide Summary
I'd like to propose a new rule for hour-long lectures and/or small groups: if you can't summarize what you taught in a single, relatively uncluttered slide, you've tried to teach too much.
Medicine involves a lot of learning and for someone who enjoys learning new things, that's great! Yet, I find I get presented with more information that I actually learn and, of the material I do learn, not much gets retained far beyond the exam.
Yesterday, I went to an informal education session, something outside the official curriculum, but one with value (I believe) to my career as a physician. It wasn't an overly simple session and there was quite a bit of information presented, but it was logically organized with some key learning points. The best part for me was the final slide, which essentially summarized the major lessons of the entire hour. More than a few details were left out of this slide, but because that core knowledge was so clearly presented and easy to memorize, those details were easier to recall.
Medical education - as well as education in general - often forgets to employ the basics of learning in their lessons. Repetition, contextual learning, patterning, scaffolding, even simple things like storytelling, these are poorly utilized in medical education. Over the long term, these concepts are employed, but that seems to be as much by accident as design. What I learn now will be applied in clerkship and residency, but the expectation appears to be that we'll know much of the pre-clerkship material by the time we start clerkship, which of course, isn't the case.
I like the idea of a single slide summary because it slows down the learning a bit. You can't put a lecture full of details or new concepts if you have to summarize it cleanly in one slide. To fill that time, you have to repeat core knowledge a few times, present it in a bit of a different context, or tell a story about how that knowledge is relevant. It forces teachers to actually teach, rather than simply transmit information. We could use a little less information transmission and a little more teaching.
Tuesday, 24 March 2015
Stress Management
So, this blog in many ways is a form of stress-relief for me. That's why the posts range from somewhat meaningless reflections on life to what I hope are some fairly serious discussions of topics in medicine, health policy, or medical education.
I tried doing a serious-only blog a while back. It died pretty quickly. The motivation to keep producing content slowly withered and it became a source of stress in its own right.
This blog has managed to survive with me still enjoying doing it for about two months now, in part because I've stopped caring about what I post and whether it's exceptionally high quality. I mention this because early today, I felt comfortable enough with this blog to make it a bit more public, to actually direct people to it. I have no idea if what I'm doing is valuable to anyone else. I hope it is. But if it's not, I'll probably keep doing this anyway.
Writing is a great outlet for worries, frustrations, annoyances, or just random thoughts that need an outlet. At this point, any benefits beyond that are just a bonus.
I tried doing a serious-only blog a while back. It died pretty quickly. The motivation to keep producing content slowly withered and it became a source of stress in its own right.
This blog has managed to survive with me still enjoying doing it for about two months now, in part because I've stopped caring about what I post and whether it's exceptionally high quality. I mention this because early today, I felt comfortable enough with this blog to make it a bit more public, to actually direct people to it. I have no idea if what I'm doing is valuable to anyone else. I hope it is. But if it's not, I'll probably keep doing this anyway.
Writing is a great outlet for worries, frustrations, annoyances, or just random thoughts that need an outlet. At this point, any benefits beyond that are just a bonus.
Minor Pre-Residency Rant
So our school just had a Career Day, where all the program directors and quite a few residents came out to talk about the residency programs at our school with us medical students. It was really well done and everyone I spoke to was extremely helpful. I came out of it feeling like I knew at least somewhat where I stood at each of the specialties I'm interested in here. Since I would prefer to stay in this city for my residency, that becomes extraordinarily useful information. I can't say enough about how much events like this help me as a student.
However, one element that really stuck out for me - and one which I've been worried about since I got accepted to Medical School - is that most programs really care about showing a deep interest in their field.
On the face of it, that makes sense, but there's a bit of a dilemma at this stage, and it goes a bit like this:
Step 1: Acknowledge the need to show interest in the specialties I'm genuinely interested in.
Step 2: Realize I don't know exactly what specialties I'm genuinely interested in.
Step 3: Do some activities in specialties I think I'm genuinely interested in.
Step 4: Find out through those activities that I'm not actually as interested in some of those specialties as I initially thought.
Step 5: Panic, because now I've expressed interest in specialties that I might not actually want.
Step 6: Panic more, because I haven't expressed enough interest in specialties that may now be higher up on my preferred list of specialties to match to, but now have no time to do it.
Step 7: Weep softly in the fetal position.
The crux of the problem is that it's quite difficult to figure out what you want to match to and the most useful information on that front comes in Clerkship and Electives, when it's often too late to do anything significant to express interest in fields you haven't already, such as doing research within that specialty. Programs want commitment on students' part well before they commit to students and even before commitments can be realistically made.
Right now, I have a number of commitments and I think I can show some interest in every field I care about at this point - and I think I've managed to narrow it down pretty well. Yet, because I start some projects in fields that I'm not considering very highly anymore, I'm a bit constrained. I want to show deeper interest in the specialties I still care about, but have no time. Research is the big one - I've got two significant research projects on the go, but because they're not directly in the specialties I'm now looking at, I worry they may not count for as much as they could.
Yet, for all that doom-and-gloom, many residents I've spoken to have told me they really figured out their specialty in 3rd year. They all managed to match, so there's got to be a way. In 3rd year, once my preferences become a bit more clear, I'll have to start to go all-out for whatever specialty I settle on. I just hope that'll be enough.
However, one element that really stuck out for me - and one which I've been worried about since I got accepted to Medical School - is that most programs really care about showing a deep interest in their field.
On the face of it, that makes sense, but there's a bit of a dilemma at this stage, and it goes a bit like this:
Step 1: Acknowledge the need to show interest in the specialties I'm genuinely interested in.
Step 2: Realize I don't know exactly what specialties I'm genuinely interested in.
Step 3: Do some activities in specialties I think I'm genuinely interested in.
Step 4: Find out through those activities that I'm not actually as interested in some of those specialties as I initially thought.
Step 5: Panic, because now I've expressed interest in specialties that I might not actually want.
Step 6: Panic more, because I haven't expressed enough interest in specialties that may now be higher up on my preferred list of specialties to match to, but now have no time to do it.
Step 7: Weep softly in the fetal position.
The crux of the problem is that it's quite difficult to figure out what you want to match to and the most useful information on that front comes in Clerkship and Electives, when it's often too late to do anything significant to express interest in fields you haven't already, such as doing research within that specialty. Programs want commitment on students' part well before they commit to students and even before commitments can be realistically made.
Right now, I have a number of commitments and I think I can show some interest in every field I care about at this point - and I think I've managed to narrow it down pretty well. Yet, because I start some projects in fields that I'm not considering very highly anymore, I'm a bit constrained. I want to show deeper interest in the specialties I still care about, but have no time. Research is the big one - I've got two significant research projects on the go, but because they're not directly in the specialties I'm now looking at, I worry they may not count for as much as they could.
Yet, for all that doom-and-gloom, many residents I've spoken to have told me they really figured out their specialty in 3rd year. They all managed to match, so there's got to be a way. In 3rd year, once my preferences become a bit more clear, I'll have to start to go all-out for whatever specialty I settle on. I just hope that'll be enough.
Why Brain, Why?!
So I woke up at 4am for absolutely no reason. Completely alert, no chance of getting back to sleep. I hate my brain.
I probably spend too much time on the computer or on my phone late at night... Sleep hygiene - it matters!
I probably spend too much time on the computer or on my phone late at night... Sleep hygiene - it matters!
Saturday, 21 March 2015
How Admissions Process Fail
I wrote briefly about a somewhat common argument in defense of current medical school admissions that doesn't quite hold up to scrutiny. Put simply, because there are so many qualified applicants to medical schools in Canada, it's not hard to design a system that selects mostly qualified applicants.
What is much harder to do is select the most qualified candidates and to do so fairly such that people aren't looked over for factors largely out of their control. Right now most medical schools' admissions processes do a reasonable job - the highly qualified candidates seem to get in with relative reliability and no one seems completely unqualified to be a future physician among the medical students I've met. Yet, there's a huge swath of applicants who are neither incredibly competent nor clearly inept. It's selecting between these candidates where the challenge lies and where I believe our current systems fall flat.
How Admissions Are Unfair
The admissions process gets accused of unfairness often, quite frequently for spurious reasons related to individual applicants not getting in (and then calling the system unfair because of it). One way in which there appears to be a clear level of unfairness, however, is in socioeconomic status.
Today's medical students come from predominantly upper-middle or upper class families. Many have physicians as parents. Being rich and connected doesn't get you into medicine - no one cares in an interview if your dad is the Head of Neurosurgery or something - but not being rich or connected can certainly play a role in keeping you out.
Medical schools obviously don't ask for your parent's income when you apply, but the factors they do look at can be greatly influenced by income and connections. In Canada, schools generally consider four major factors in granting admission: GPA, MCAT, extra-curriculars (ECs), and interviews.
GPA requires consistently high marks. Sometimes a single bad mark can ruin an applicant's chances at select schools. Even at schools that have relatively low GPA requirements, you need pretty close to straight-A's. That level of consistency requires time and energy. That's reasonable if you have nothing to do aside from school, but becomes a real challenge if you're commuting from home, working significant hours (even 10+ per week has been shown to decrease academic performance), or have domestic responsibilities. Money can also buy some extra help - hiring a tutor or doing some difficult courses part-time during the summer when you can afford to put some extra time in (or when schools don't consider them in your GPA) are all pathways unavailable to lower-income students. Not to mention that undergraduate education isn't exactly cheap...
ECs are much the same - they take time and energy. Some ECs also take money, such as travel abroad or high-level sports. There is a push to better consider activities and experiences that reflect life for lower-income students, such as valuing work experience or time spent caring for family members. There is also a trend against ECs that are clearly bought, not earned, such as travelling abroad for so-called "voluntourism" initiatives. Still, there is plenty of room for bias. A job in a research lab looks much better than a job in retail, yet lab jobs often don't have enough hours or sufficient flexibility for some students to manage. They also tend to require high marks. Connections make a difference too - those who have physicians as parents are more likely to be aware of opportunities in undergrad and may have an advantage in obtaining those coveted positions.
The MCAT also requires time and money, though I'd argue less than maintaining a high GPA or developing strong ECs. The financial cost for me to write my MCAT, including prep materials, was somewhere in the range of $500, plus about 4 weeks of dedicated studying, compared to tens of thousands of dollars and 4 years needed for an undergrad. Still, my experience may not be universal and there are definitely individuals who spend exorbitant amounts to prepare for the MCAT, or who write it multiple times to get a better score. If these expenses are even modestly helpful, it's yet another barrier for low-income students.
Interviews are probably the one chance to equal out the field a bit. People are persuaded by stories of struggle and interviews are the perfect opportunity for lower-income applicants to put what they've done in proper context. Yet, interviews come only after all the other factors are considered. Interviews do have some barriers as well - clothing and travel. Suits and other forms of formal wear are expensive! So is travelling to interviews, which can be halfway across our rather large country for some. For many students, it's a small expense, but when you're living paycheque-to-paycheque, it's not.
Admittedly, factors related to competence are likely at play here. Intelligence correlates with income and has a hereditary component meaning the offspring of wealthy individuals are more likely to be sufficiently intelligent than those from non-wealthy families. However, the disparity is striking. In light of the financial barriers to entering medical school, I'm doubtful that these sort of correlations explain the whole picture.
All of the factors medical schools consider have support as mechanisms to evaluate qualifications. Yet, because they reflect more than qualifications, particularly personal circumstances, they tend to cut out those with challenges beyond their control to overcome.
How Admissions Fail To Capture The Best Candidates
In providing unintentional preference to wealthy applicants, medical schools automatically miss out on some very capable individuals. Yet even among those from similar socioeconomic backgrounds, there are ways in which the current system selects candidates who may not be the best qualified.
Schools want the smartest, hardest working, most responsible candidates. Patients want physicians who are ethical, caring, and who have strong communication skills. I'd argue these six attributes are essentially what admissions committees are trying to measure.
GPA and the MCAT largely cover what schools wants - intelligence and work ethic. ECs can hit everything somewhat depending on the types of ECs done. Interviews are primarily meant to assess ethics and communication skills.
Ideally, we want applicants to be exceptionally strong in all these attributes. If they are, they tend to do quite well in all the admission criteria - stellar GPA, high MCAT scores, varied and unique ECs, plus a solid interview. Very few people fit this mold. Deciding between individuals who are not stellar in all categories is trickier. Is someone with a 4.0 GPA but a 50th percentile MCAT more qualified than someone with a 99th percentile MCAT but a 3.5 GPA? Some schools in Canada say yes. Others say no.
I'd argue both are probably smart enough to be a physician and it's the other factors that should be analyzed. Unfortunately, most schools in Canada don't allow for strength in one category to make up for strength in another, even when measuring roughly the same metrics. This leaves a lot of individuals cut out of consideration relatively arbitrarily. It's one thing to take a look at an applicant and ultimately decide against them - it's another to dismiss an applicant without looking at them at all. Yet, that's what virtually every medical school does. In Canada, the main barrier to entry into medical school is having high enough stats (GPA and MCAT) for schools to bother looking at the rest of your application. Once that bar is cleared, entry into medical school is very likely, even if it takes a few application cycles. In effect, this means that GPA and MCAT dictate entry into the profession, even though ECs and interview scores are considered.
In some respects, the variation in criteria for medical schools in Canada does allow for a bit of a bigger net to be cast. Ottawa, for example, has crazy-high GPA requirements, but doesn't care about the MCAT at all. Western, by contrast, has insane MCAT requirements, but fairly lax GPA cutoffs. Individually these two schools ignore a lot of qualified applicants, but together they're at least looking at wider number of qualified applicants.
Nevertheless, GPA and MCAT still reign king. ECs and interviews seem to matter only when exceptionally deficient. This leads to schools largely getting the students they want - smart, hard-working ones. Patients, who want ethical, caring, communicative individuals tend to lose out. Looser requirements for GPA and MCAT, looking at more applicants' non-academic qualifications, may allow those qualifications to matter a bit more.
I've yet to meet a medical student or physician too dumb for the job, but I've met plenty who lacked the soft skills to be capable. Our admissions process is part of that.
What is much harder to do is select the most qualified candidates and to do so fairly such that people aren't looked over for factors largely out of their control. Right now most medical schools' admissions processes do a reasonable job - the highly qualified candidates seem to get in with relative reliability and no one seems completely unqualified to be a future physician among the medical students I've met. Yet, there's a huge swath of applicants who are neither incredibly competent nor clearly inept. It's selecting between these candidates where the challenge lies and where I believe our current systems fall flat.
How Admissions Are Unfair
The admissions process gets accused of unfairness often, quite frequently for spurious reasons related to individual applicants not getting in (and then calling the system unfair because of it). One way in which there appears to be a clear level of unfairness, however, is in socioeconomic status.
Today's medical students come from predominantly upper-middle or upper class families. Many have physicians as parents. Being rich and connected doesn't get you into medicine - no one cares in an interview if your dad is the Head of Neurosurgery or something - but not being rich or connected can certainly play a role in keeping you out.
Medical schools obviously don't ask for your parent's income when you apply, but the factors they do look at can be greatly influenced by income and connections. In Canada, schools generally consider four major factors in granting admission: GPA, MCAT, extra-curriculars (ECs), and interviews.
GPA requires consistently high marks. Sometimes a single bad mark can ruin an applicant's chances at select schools. Even at schools that have relatively low GPA requirements, you need pretty close to straight-A's. That level of consistency requires time and energy. That's reasonable if you have nothing to do aside from school, but becomes a real challenge if you're commuting from home, working significant hours (even 10+ per week has been shown to decrease academic performance), or have domestic responsibilities. Money can also buy some extra help - hiring a tutor or doing some difficult courses part-time during the summer when you can afford to put some extra time in (or when schools don't consider them in your GPA) are all pathways unavailable to lower-income students. Not to mention that undergraduate education isn't exactly cheap...
ECs are much the same - they take time and energy. Some ECs also take money, such as travel abroad or high-level sports. There is a push to better consider activities and experiences that reflect life for lower-income students, such as valuing work experience or time spent caring for family members. There is also a trend against ECs that are clearly bought, not earned, such as travelling abroad for so-called "voluntourism" initiatives. Still, there is plenty of room for bias. A job in a research lab looks much better than a job in retail, yet lab jobs often don't have enough hours or sufficient flexibility for some students to manage. They also tend to require high marks. Connections make a difference too - those who have physicians as parents are more likely to be aware of opportunities in undergrad and may have an advantage in obtaining those coveted positions.
The MCAT also requires time and money, though I'd argue less than maintaining a high GPA or developing strong ECs. The financial cost for me to write my MCAT, including prep materials, was somewhere in the range of $500, plus about 4 weeks of dedicated studying, compared to tens of thousands of dollars and 4 years needed for an undergrad. Still, my experience may not be universal and there are definitely individuals who spend exorbitant amounts to prepare for the MCAT, or who write it multiple times to get a better score. If these expenses are even modestly helpful, it's yet another barrier for low-income students.
Interviews are probably the one chance to equal out the field a bit. People are persuaded by stories of struggle and interviews are the perfect opportunity for lower-income applicants to put what they've done in proper context. Yet, interviews come only after all the other factors are considered. Interviews do have some barriers as well - clothing and travel. Suits and other forms of formal wear are expensive! So is travelling to interviews, which can be halfway across our rather large country for some. For many students, it's a small expense, but when you're living paycheque-to-paycheque, it's not.
Admittedly, factors related to competence are likely at play here. Intelligence correlates with income and has a hereditary component meaning the offspring of wealthy individuals are more likely to be sufficiently intelligent than those from non-wealthy families. However, the disparity is striking. In light of the financial barriers to entering medical school, I'm doubtful that these sort of correlations explain the whole picture.
All of the factors medical schools consider have support as mechanisms to evaluate qualifications. Yet, because they reflect more than qualifications, particularly personal circumstances, they tend to cut out those with challenges beyond their control to overcome.
How Admissions Fail To Capture The Best Candidates
In providing unintentional preference to wealthy applicants, medical schools automatically miss out on some very capable individuals. Yet even among those from similar socioeconomic backgrounds, there are ways in which the current system selects candidates who may not be the best qualified.
Schools want the smartest, hardest working, most responsible candidates. Patients want physicians who are ethical, caring, and who have strong communication skills. I'd argue these six attributes are essentially what admissions committees are trying to measure.
GPA and the MCAT largely cover what schools wants - intelligence and work ethic. ECs can hit everything somewhat depending on the types of ECs done. Interviews are primarily meant to assess ethics and communication skills.
Ideally, we want applicants to be exceptionally strong in all these attributes. If they are, they tend to do quite well in all the admission criteria - stellar GPA, high MCAT scores, varied and unique ECs, plus a solid interview. Very few people fit this mold. Deciding between individuals who are not stellar in all categories is trickier. Is someone with a 4.0 GPA but a 50th percentile MCAT more qualified than someone with a 99th percentile MCAT but a 3.5 GPA? Some schools in Canada say yes. Others say no.
I'd argue both are probably smart enough to be a physician and it's the other factors that should be analyzed. Unfortunately, most schools in Canada don't allow for strength in one category to make up for strength in another, even when measuring roughly the same metrics. This leaves a lot of individuals cut out of consideration relatively arbitrarily. It's one thing to take a look at an applicant and ultimately decide against them - it's another to dismiss an applicant without looking at them at all. Yet, that's what virtually every medical school does. In Canada, the main barrier to entry into medical school is having high enough stats (GPA and MCAT) for schools to bother looking at the rest of your application. Once that bar is cleared, entry into medical school is very likely, even if it takes a few application cycles. In effect, this means that GPA and MCAT dictate entry into the profession, even though ECs and interview scores are considered.
In some respects, the variation in criteria for medical schools in Canada does allow for a bit of a bigger net to be cast. Ottawa, for example, has crazy-high GPA requirements, but doesn't care about the MCAT at all. Western, by contrast, has insane MCAT requirements, but fairly lax GPA cutoffs. Individually these two schools ignore a lot of qualified applicants, but together they're at least looking at wider number of qualified applicants.
Nevertheless, GPA and MCAT still reign king. ECs and interviews seem to matter only when exceptionally deficient. This leads to schools largely getting the students they want - smart, hard-working ones. Patients, who want ethical, caring, communicative individuals tend to lose out. Looser requirements for GPA and MCAT, looking at more applicants' non-academic qualifications, may allow those qualifications to matter a bit more.
I've yet to meet a medical student or physician too dumb for the job, but I've met plenty who lacked the soft skills to be capable. Our admissions process is part of that.
Friday, 20 March 2015
Transitions
Hitting an interesting point in my pre-clerkship training right now.
We just finished two blocks that I really enjoyed, somewhat unexpectedly. MSK was great - I feel like I learned a lot, but never felt overwhelmed. I don't expect to go into a MSK-focused field like orthopedics or physiatry, so I didn't go into the course anticipating that I'd find it all that interesting, but I really did. Most of what I am looking at will involve some sort of MSK knowledge, so I'll take that as a win.
We also had a short Emergency Medicine block. I loved it. Every part of it. The underlying knowledge base I find fascinating, the clinical decision-making seems logically and useful, while its role in medicine intrigues me more than I thought it would. I'm now seriously considering emergency medicine as a specialty, after I had all but written it off.
Yet, we're now entering the final two blocks of my pre-clerkship training: Neurology and Psychiatry. I will not be a neurologist or psychiatrist. I do find some of these fields very interesting, but they're mixed with other aspects I find overly tedious. There's a lot of detail-oriented material with questionable relevance to clinical practice. These will be tough blocks to get through, especially with clerkship so close.
It's going to be a real challenge to stay focused on the classroom when all I want to do is get into the clinical setting. About all I can do at this point is to tell myself that I just need to get past these two final blocks and then the fun can start. Home stretch!
Monday, 16 March 2015
March Break Ending...
It's the end of March Break. I got a fair bit done over this week, but for the most part, I was just exceptionally lazy. Played video games and watched a lot of TV.
At first I felt guilty - I've got a lot I should be doing! But hey, a lot of my fellow classmates go on vacation during this time. I'll be satisfied with a moderately productive staycation this time around.
At first I felt guilty - I've got a lot I should be doing! But hey, a lot of my fellow classmates go on vacation during this time. I'll be satisfied with a moderately productive staycation this time around.
Sunday, 15 March 2015
Paying For Healthcare (Part II)
A while back, I talked about the importance of trying to keep healthcare costs as low as reasonably achievable. Today, I'll try to delve into the much more difficult discussion of how that might be accomplished.
Reducing healthcare costs, or at least slowing the rise in those costs, is a tricky proposition. These costs have grown faster than inflation for a reason - controlling healthcare expenditures is hard! Certainly, if I had an amazing insight into how to accomplish the goal of reduced healthcare costs, I wouldn't be posting it on a blog - I'd be selling my consulting services to the government or insurance companies or hospitals.
However, when you break it down, there's really only two ways to keep costs down. Healthcare can be broken down as a set of discrete services, so we either need to reduce the total quantity of services provided, or we need to reduce the cost per service provided.
Reducing Quantity of Services Provided
The principle here is fairly simple. If you want to spend less money on say, antibiotics, simply prescribe fewer antibiotics! Or better yet, prescribe no antibiotics, ever. Of course, antibiotics have value - many infections are untreatable without them. Not using them at all would be a very bad idea.
Yet, there are some situations where antibiotics are unnecessary or even harmful. Simple, acute upper respiratory infections, for example, are often viral, for which antibiotics do nothing. Prescribing antibiotics for such an infection is very likely to be useless (there's also some evidence that even with bacterial infections, they're not very useful either, though this is a somewhat more complex area of discussion). Eliminating prescriptions of these antibiotics would save money without significantly impacting health. The Choosing Wisely Campaign attempts to address this sort of waste. Both American and Canadian campaigns have sprung up to encourage physicians - and to a lesser extent, patients - to be more discriminating about what medical services they actually necessary and when to employ them.
There are also some more limited instances where a service in healthcare is entirely unnecessary. Apparently we used to intentionally put people into comas by overdosing them with insulin. That wasn't a great idea... Eliminating useless or harmful services also saves money. While it's much harder to tell that a particular diagnostic test or therapy is completely useless for all people in all circumstances, there are almost certainly some of these services being employed in mainstream medicine today. Identifying these practices is worthwhile from both a medical and economic perspective.
Reducing Cost of Services Provided
While lowering the quantity of services is relatively straight-forward as a concept, reducing costs of each service is not.
What goes into the cost of a healthcare test or treatment is complex, but again, we can break it down into components - personnel, supplies, and durable equipment (including facilities).
1) Personnel
Healthcare takes people to work. Lots of people! People-heavy fields are expensive though and healthcare is no exception. That almost everyone in medicine is generally well-educated adds to this cost. There are a wide variety of professions within the healthcare system, but I'll focus on physicians. Physicians are moderately numerous and get paid a lot. Even small percentage reductions in numbers or salaries of physicians can meaningfully reduce healthcare costs.
Having fewer physicians is a non-starter. Each physician and there are already widespread concerns about overworking these providers. Physicians will increase significantly in number as medical schools have increased their class sizes to keep up with demand. That leaves salaries. Again, physicians receive good compensation. After overhead but before tax, most physicians make $200,000 a year. A few make a bit less, many make significantly more.
Reducing physician salaries, while hardly a sustainable strategy for minimizing healthcare costs, can be part of the solution. That's what the Ontario government did.
2) Supplies
There are numerous supplies that get used once in medicine and then tossed or consumed. There are often good reasons for this - we're not going to reuse needles, for example - but nevertheless, there are certainly instances where we overuse supplies or use supplies that are more expensive than necessary. For example, I did an observership in a clinical teaching unit (CTU) which naturally had many learners. We saw nearly a dozen patients, all of whom had some sort of communicable disease, but most without anything really all that serious or likely to spread. Yet, all 5 or so of us doing rounds put on full protective equipment, even though half of us just stood in the back, well away from the patients. Meanwhile family members pop in and out of the room with no equipment whatsoever. Me wearing that equipment is hospital policy and that policy exists for a good reason - but in this case I probably cost the hospital at least $20 without much in the way of appreciable benefit to them, the patients, or myself.
The major consumable supply in healthcare, however, is pharmaceuticals. We spend a lot on drugs. And a fair bit of that expense is likely unnecessary. Too many name-brand drugs ordered when generics would be just as effective. Physicians may prescribe too many antidepressants, too many anti-psychotics, too many antibiotics, too many ADHD medications, and too many statins, just to name a few. Fewer drugs prescribed means lower healthcare costs.
If you can still treat people effectively without using as many medications or other supplies or other supplies, costs are likely to fall. This is sometimes a bit hard to untangle from the above discussion of simply reducing services and there is a bit of crossover here, but conceptually, the goal is to provide the same treatment (i.e. addressing the patient's medical concerns), only with cheaper, fewer, or no drugs.
3) Durable Equipment
Last, but not least, we have the stuff that sticks around for a while. This can range from something as simple as my stethoscope, to the giant hospitals where I will do most of my training. There's not a lot of low-hanging fruit here to pick on, because generally durable equipment are fairly big, one-time expenditures that last for at least a decade, so a fair bit of thought gets put into them. I spent a ton of time researching what stethoscope was right for my needs. Likewise, no one builds a hospital on a whim.
If there are costs to be saved here, it's likely in the utilization of these durable goods and finding ways to encourage practices that draw on lower-cost durable goods, which often goes hand-in-hand with reductions in personnel or supplies costs. For example, outpatient clinics generally require less infrastructure than inpatient wards. Doing more outpatient work saves on infrastructure costs (though it saves a lot more in day-to-day costs). An MRI machine costs well over a million dollars, while ultrasound machines cost less than $100k - if we can get away with doing more ultrasounds and fewer MRIs, then we probably save on equipment costs by buying fewer MRI machines.
Closing Thoughts
I've given a fairly simplistic rundown of some of the major ways in which healthcare spending could be reduced. While I hope I've given a good sense of what could be done, I haven't really touched on the how these approaches could be accomplished. That requires a much more complex discussion of government policy, economics, legal considerations, and human psychology.
I also haven't discussed the drawbacks to slashing spending - and there certainly are some. Whenever you try to cut away the bad expenditures, you risk cutting away some good ones as well. It's undeniably true that antibiotics are over-prescribed in some cases, but people often need antibiotics! There's always a chance that in stopping needless use of antibiotics, some people will not get them when it is appropriate.
Similarly, every action has unintended, sometimes undesired secondary effects. Cutting physician salaries saves money, but if it reduces access to the healthcare system, it may result in sicker people who require more expensive services down the road. There are certainly methods to anticipate and minimize unwanted secondary effects, but no change is made in a vacuum and it can be hard to predict what the full effect of a policy change will be in 10+ years.
It's a complicated discussion and while I've tried to simply the problem, there are no simple answers. Yet, as a physician-in-training, I believe it's an important one - for the sake of my profession, my future patients, and for my community as a whole.
Reducing healthcare costs, or at least slowing the rise in those costs, is a tricky proposition. These costs have grown faster than inflation for a reason - controlling healthcare expenditures is hard! Certainly, if I had an amazing insight into how to accomplish the goal of reduced healthcare costs, I wouldn't be posting it on a blog - I'd be selling my consulting services to the government or insurance companies or hospitals.
However, when you break it down, there's really only two ways to keep costs down. Healthcare can be broken down as a set of discrete services, so we either need to reduce the total quantity of services provided, or we need to reduce the cost per service provided.
Reducing Quantity of Services Provided
The principle here is fairly simple. If you want to spend less money on say, antibiotics, simply prescribe fewer antibiotics! Or better yet, prescribe no antibiotics, ever. Of course, antibiotics have value - many infections are untreatable without them. Not using them at all would be a very bad idea.
Yet, there are some situations where antibiotics are unnecessary or even harmful. Simple, acute upper respiratory infections, for example, are often viral, for which antibiotics do nothing. Prescribing antibiotics for such an infection is very likely to be useless (there's also some evidence that even with bacterial infections, they're not very useful either, though this is a somewhat more complex area of discussion). Eliminating prescriptions of these antibiotics would save money without significantly impacting health. The Choosing Wisely Campaign attempts to address this sort of waste. Both American and Canadian campaigns have sprung up to encourage physicians - and to a lesser extent, patients - to be more discriminating about what medical services they actually necessary and when to employ them.
There are also some more limited instances where a service in healthcare is entirely unnecessary. Apparently we used to intentionally put people into comas by overdosing them with insulin. That wasn't a great idea... Eliminating useless or harmful services also saves money. While it's much harder to tell that a particular diagnostic test or therapy is completely useless for all people in all circumstances, there are almost certainly some of these services being employed in mainstream medicine today. Identifying these practices is worthwhile from both a medical and economic perspective.
Reducing Cost of Services Provided
While lowering the quantity of services is relatively straight-forward as a concept, reducing costs of each service is not.
What goes into the cost of a healthcare test or treatment is complex, but again, we can break it down into components - personnel, supplies, and durable equipment (including facilities).
1) Personnel
Healthcare takes people to work. Lots of people! People-heavy fields are expensive though and healthcare is no exception. That almost everyone in medicine is generally well-educated adds to this cost. There are a wide variety of professions within the healthcare system, but I'll focus on physicians. Physicians are moderately numerous and get paid a lot. Even small percentage reductions in numbers or salaries of physicians can meaningfully reduce healthcare costs.
Having fewer physicians is a non-starter. Each physician and there are already widespread concerns about overworking these providers. Physicians will increase significantly in number as medical schools have increased their class sizes to keep up with demand. That leaves salaries. Again, physicians receive good compensation. After overhead but before tax, most physicians make $200,000 a year. A few make a bit less, many make significantly more.
Reducing physician salaries, while hardly a sustainable strategy for minimizing healthcare costs, can be part of the solution. That's what the Ontario government did.
2) Supplies
There are numerous supplies that get used once in medicine and then tossed or consumed. There are often good reasons for this - we're not going to reuse needles, for example - but nevertheless, there are certainly instances where we overuse supplies or use supplies that are more expensive than necessary. For example, I did an observership in a clinical teaching unit (CTU) which naturally had many learners. We saw nearly a dozen patients, all of whom had some sort of communicable disease, but most without anything really all that serious or likely to spread. Yet, all 5 or so of us doing rounds put on full protective equipment, even though half of us just stood in the back, well away from the patients. Meanwhile family members pop in and out of the room with no equipment whatsoever. Me wearing that equipment is hospital policy and that policy exists for a good reason - but in this case I probably cost the hospital at least $20 without much in the way of appreciable benefit to them, the patients, or myself.
The major consumable supply in healthcare, however, is pharmaceuticals. We spend a lot on drugs. And a fair bit of that expense is likely unnecessary. Too many name-brand drugs ordered when generics would be just as effective. Physicians may prescribe too many antidepressants, too many anti-psychotics, too many antibiotics, too many ADHD medications, and too many statins, just to name a few. Fewer drugs prescribed means lower healthcare costs.
If you can still treat people effectively without using as many medications or other supplies or other supplies, costs are likely to fall. This is sometimes a bit hard to untangle from the above discussion of simply reducing services and there is a bit of crossover here, but conceptually, the goal is to provide the same treatment (i.e. addressing the patient's medical concerns), only with cheaper, fewer, or no drugs.
3) Durable Equipment
Last, but not least, we have the stuff that sticks around for a while. This can range from something as simple as my stethoscope, to the giant hospitals where I will do most of my training. There's not a lot of low-hanging fruit here to pick on, because generally durable equipment are fairly big, one-time expenditures that last for at least a decade, so a fair bit of thought gets put into them. I spent a ton of time researching what stethoscope was right for my needs. Likewise, no one builds a hospital on a whim.
If there are costs to be saved here, it's likely in the utilization of these durable goods and finding ways to encourage practices that draw on lower-cost durable goods, which often goes hand-in-hand with reductions in personnel or supplies costs. For example, outpatient clinics generally require less infrastructure than inpatient wards. Doing more outpatient work saves on infrastructure costs (though it saves a lot more in day-to-day costs). An MRI machine costs well over a million dollars, while ultrasound machines cost less than $100k - if we can get away with doing more ultrasounds and fewer MRIs, then we probably save on equipment costs by buying fewer MRI machines.
Closing Thoughts
I've given a fairly simplistic rundown of some of the major ways in which healthcare spending could be reduced. While I hope I've given a good sense of what could be done, I haven't really touched on the how these approaches could be accomplished. That requires a much more complex discussion of government policy, economics, legal considerations, and human psychology.
I also haven't discussed the drawbacks to slashing spending - and there certainly are some. Whenever you try to cut away the bad expenditures, you risk cutting away some good ones as well. It's undeniably true that antibiotics are over-prescribed in some cases, but people often need antibiotics! There's always a chance that in stopping needless use of antibiotics, some people will not get them when it is appropriate.
Similarly, every action has unintended, sometimes undesired secondary effects. Cutting physician salaries saves money, but if it reduces access to the healthcare system, it may result in sicker people who require more expensive services down the road. There are certainly methods to anticipate and minimize unwanted secondary effects, but no change is made in a vacuum and it can be hard to predict what the full effect of a policy change will be in 10+ years.
It's a complicated discussion and while I've tried to simply the problem, there are no simple answers. Yet, as a physician-in-training, I believe it's an important one - for the sake of my profession, my future patients, and for my community as a whole.
Wednesday, 11 March 2015
Fairness in Medical School Admissions
A favourite topic of mine is medical education and one of the more interesting aspects of medical education to me is admissions. In our current system, admission to Medical School is the major choke-point. Before you get that admission, you're not going to become a doctor. Once you get that admission, you are almost guaranteed to become a physician. It's a fairly important milestone.
It's also a very difficult milestone to get beyond. Medical school admissions, particularly in Canada, are insanely competitive. Just getting the GPA/MCAT combo to get looked at is a non-trivial task. Having the more subjective measures be up-to-par is an added challenge, your extra-curriculars, letters of reference, interview performance all can matter as well. Far more people apply than gain admissions and there's a large set of interested individuals who never bother to apply at all, knowing it would be futile.
Because admissions is the major choke-point to entering the profession, having an effective and fair admissions process is a meaningful concern. At some point, I'd like to dig into the nuances of this process in depth, probably over several posts. For now, I'll stick to commenting on one point that always bugs me: just because we have generally good physicians does not mean that we have a good admissions process.
The thing is, far more qualified individuals want to be physicians than are allowed to be physicians. Ontario takes approximately 1000 new medical students each year, most of whom will likely be very good physicians. Yet, there are several more thousand aspiring physicians who cannot gain admissions who would probably be good physicians as well. This leaves plenty of room for inefficiency, inequality, or in some cases, downright inequality in the selection process.
Here's a simple scenario - let's say you have three applicants for one medical school position, Jim, Bob, and Ray.
Jim is not qualified to be a physician, not even close. Both Bob and Ray, however, would probably make good physicians. Jim and Bob are both tall, but Ray is not.
A selection process that considers both height and qualifications would select Bob. Bob's qualified, so that's not a bad outcome for the system - at least we're not getting Jim! But it's not a fair system to Ray, who's also qualified, but doesn't happen to be tall, a factor which isn't relevant or within Ray's control.
The current admission systems are rarely so obviously preferential, but bias can still creep in. If there were 100 Jims and 100 Bobs and 100 Rays applying for 100 positions, without any stated preference for height, yet we ended up with 90 Bobs and 10 Rays, that's not likely to be a fair system. Sure, we didn't end up with any Jims, so height doesn't trump qualifications, but that's a small comfort to the many Rays who got passed over for Bobs when the only major difference between them is height.
With so many qualified applicants, it's not too hard to avoid the unqualified ones (though the odd one still slips through the cracks...). But that's not good enough, not for patients, and not for applicants who deserve a fair shot at the profession.
Tuesday, 10 March 2015
Stress Management
I took on too much this year. Not way too much, just a bit more than I should have, and at times it stretches me a bit thin. This causes some stress. Not a ton - I'm still staying on top of everything, I maintain some semblance of a social life and I do get to spend a fair bit of time at home with my significant other.
Stress management for me takes many forms, but the main one is just letting my brain sort through the dozens of thoughts in it. Sometimes this means some alone time, just bouncing ideas around. Sometimes this means discussing what's rattling around in my head with friends, family, colleagues, or even the dog (the dog is a very good listener when he's not stealing socks).
One of the main purposes of this blog is stress management. It lets me get those thoughts out without avoiding the world or overwhelming those around me. I find writing (well, typing) to be fairly relaxing as well. So, at times you'll see me writing about tiny, insignificant things that have little if anything to do with medicine. Sometimes I'll write diatribes about a very specific topic in health care. It all depends what's stuck up in my brain that needs to come out.
My hope is that between all these outpourings of random thoughts, there will be some useful bits for those reading, if there is anyone reading.
Stress management for me takes many forms, but the main one is just letting my brain sort through the dozens of thoughts in it. Sometimes this means some alone time, just bouncing ideas around. Sometimes this means discussing what's rattling around in my head with friends, family, colleagues, or even the dog (the dog is a very good listener when he's not stealing socks).
One of the main purposes of this blog is stress management. It lets me get those thoughts out without avoiding the world or overwhelming those around me. I find writing (well, typing) to be fairly relaxing as well. So, at times you'll see me writing about tiny, insignificant things that have little if anything to do with medicine. Sometimes I'll write diatribes about a very specific topic in health care. It all depends what's stuck up in my brain that needs to come out.
My hope is that between all these outpourings of random thoughts, there will be some useful bits for those reading, if there is anyone reading.
Saturday, 7 March 2015
Webcomics
Like a lot of kids, I grew up reading comics. Not the superhero type comics (though I'm starting on those now), but the type found in the back of the newspaper, or in the funnies section. You know, back when newspapers were still a thing. Calvin & Hobbes and then Zits were the big ones.
Reading comics has stuck with me and I've been absolutely thrilled with the way comics have evolved. In the past, only a few comic strip writers could really make a career of it. Either you managed to get published in a large number of newspapers and had enough to live on, or you didn't and comics became, at most, a hobby.
These days, webcomics are supplanting the traditional print comics and it's nothing short of amazing. Most webcomics don't get their creators rich, but many provide enough to live on, particularly with the rise of crowd-funding. A couple thousand dedicated followers are enough to support an artist if they're willing to pony up a bit of cash for projects (usually books) every now and then.
The great thing about online comics is that they're relatively free of constraints. They can be about virtually anything, provided there's a natural reader base. They can take any format - and that format can change! They can publish on their own schedules, rather than what a publisher demands. This leads to some incredible of variety in the webcomic world.
I spend a bit too much time reading webcomics and draw on them frequently in life. I will likely post more than a few on this blog if they're relevant to the topic. I will try to reference them as explicitly and overtly as possible - these content creators deserve as much credit as they can get for the work they do. And I encourage anyone reading to visit their sites and check them out!
Thursday, 5 March 2015
March Break Incoming
Just finished the exam I missed because I was attending a conference and with March Break coming up, I can finally take a breath.
This semester has flown by so far. After the Christmas Break, we had one fairly intense week of class, a week of exams and then a fairly intense (but worthwhile) MSK block. Two of my clubs have been extra-busy since the break and the workload from my involvement with the school's journal has stepped up in a big way. The demands from my research project intensified a bit, though I've been lucky to have an exceptionally competent, laid-back supervisor.
I still have a ton on my plate - and because apparently I like to suffer, I seem to keep taking on more - but having a week to put it all together really does help.
I hope to sign up for the USMLEs, get my active ECs in order, set up some observerships (I've been neglecting these and I find them very worthwhile), and get my research project going a bit.
Oh, and sleep. That'd be nice.
This semester has flown by so far. After the Christmas Break, we had one fairly intense week of class, a week of exams and then a fairly intense (but worthwhile) MSK block. Two of my clubs have been extra-busy since the break and the workload from my involvement with the school's journal has stepped up in a big way. The demands from my research project intensified a bit, though I've been lucky to have an exceptionally competent, laid-back supervisor.
I still have a ton on my plate - and because apparently I like to suffer, I seem to keep taking on more - but having a week to put it all together really does help.
I hope to sign up for the USMLEs, get my active ECs in order, set up some observerships (I've been neglecting these and I find them very worthwhile), and get my research project going a bit.
Oh, and sleep. That'd be nice.
Wednesday, 4 March 2015
Paying For Healthcare
Recently, a number of events have happened - both in the wider medical community and in my little bubble - that involve how we pay for healthcare. It's a difficult subject, one that elicits a wide variety of opinions and positions.
The Fundamental Dilemma
Much of the controversy on healthcare funding comes from a relatively simple conflict, derived from two widely-held positions.
1) We value health and life more than money when it comes to us or our loved ones.
2) We value money (in the form of lower taxes and insurance premiums) more than health and life when it comes to the vast majority of people we haven't met.
Basically we care about individual health more than collective health, but since the collective is made up of individuals, we get stuck between a rock and a hard place - constant pressure to reduce total costs along with constant pressure to increase individual costs. Since many decisions on spending get made on the patient- or individual-level where the pressure to increase spending is greater, it tends to win. Hence, ever-increasing healthcare costs.
Affordability
The catch comes that many individuals can afford to pay more for healthcare. When they have the option to do so for themselves (but not others) they often do so. In the US, you see this in luxury care for those able to afford it, and medical bankruptcy for those unable to afford it. In Canada, you see this in the push for a dual-tier system, where the wealthy would be able to pay extra money for more care than provided for by the public system. For those concerned with more equal access for individuals of all socioeconomic backgrounds, the push is more for increased taxes to pay for higher-quality heathcare for all.
Mo' Money, Not Mo' Health?
I work in healthcare. I would stand to benefit significantly if we suddenly spent more on healthcare, whether through a private, dual-tier system or through increased government expenditures. Yet, more money devoted to healthcare doesn't necessarily mean better health.
The Canada-US disparity in funding expresses this fairly easily. The US pays far more for their healthcare than Canada does, yet has overall health outcomes which are, at best, equivalent. Part of that is having great care for those who can afford it, yet very low-quality care for a group who cannot afford reasonable care. Fixing that disparity could push the US ahead of Canada in standard health metrics, but even so, not by all that much (and it might not even do that).
The thing is, that much money could have a real, meaningful impact on people's health - but not if it's spent in the healthcare system. The further into this field I get, the more I realize how poor many of our diagnostic tests and therapeutic interventions are. Some are incredibly effective, but many of a middling efficacy, while a few other may not work at all. There are some interventions that we know work really well though - these are improved diet, increased exercise, quitting smoking, reducing stress, longer/improved sleep, and moderating alcohol consumption. The healthcare system is slowly beginning to focus on these highly important lifestyle factors, but because they're part of a person's lifestyle, they're affected by much more than just healthcare services.
The difference in healthcare spending between Canada and the US is about 6% of GDP. If Canada decided it could afford to spend an extra 6% of its GDP on improving health - roughly $100 billion each year - I'd much rather see it go to efforts to improve those metrics that we know work. Getting people to eat better or exercise more has always been a difficult challenge, but with $100 billion each year, I bet we could come up with a few things that'd have an impact.
This brings me to my main point - there's a reason to control costs in healthcare, because healthcare isn't the same as health and it's certainly not the same as life. We want good healthcare and I want to be part of providing it. But I want good healthcare because I want people (including myself!) to be happy and prosperous. If the costs of healthcare hinder those efforts by minimizing spending on other worthy pursuits more than they help directly by improving health, it's not really beneficial. There are diminishing returns when pumping more money into healthcare, especially when that additional money doesn't have a clearly established, useful purpose.
Bottom line - controlling health care costs, whether public costs paid through taxes or private costs paid through insurance premiums and out of pocket, is an important goal, even for those who want the healthiest people possible.
The Fundamental Dilemma
Much of the controversy on healthcare funding comes from a relatively simple conflict, derived from two widely-held positions.
1) We value health and life more than money when it comes to us or our loved ones.
2) We value money (in the form of lower taxes and insurance premiums) more than health and life when it comes to the vast majority of people we haven't met.
Basically we care about individual health more than collective health, but since the collective is made up of individuals, we get stuck between a rock and a hard place - constant pressure to reduce total costs along with constant pressure to increase individual costs. Since many decisions on spending get made on the patient- or individual-level where the pressure to increase spending is greater, it tends to win. Hence, ever-increasing healthcare costs.
Affordability
The catch comes that many individuals can afford to pay more for healthcare. When they have the option to do so for themselves (but not others) they often do so. In the US, you see this in luxury care for those able to afford it, and medical bankruptcy for those unable to afford it. In Canada, you see this in the push for a dual-tier system, where the wealthy would be able to pay extra money for more care than provided for by the public system. For those concerned with more equal access for individuals of all socioeconomic backgrounds, the push is more for increased taxes to pay for higher-quality heathcare for all.
Mo' Money, Not Mo' Health?
I work in healthcare. I would stand to benefit significantly if we suddenly spent more on healthcare, whether through a private, dual-tier system or through increased government expenditures. Yet, more money devoted to healthcare doesn't necessarily mean better health.
The Canada-US disparity in funding expresses this fairly easily. The US pays far more for their healthcare than Canada does, yet has overall health outcomes which are, at best, equivalent. Part of that is having great care for those who can afford it, yet very low-quality care for a group who cannot afford reasonable care. Fixing that disparity could push the US ahead of Canada in standard health metrics, but even so, not by all that much (and it might not even do that).
The thing is, that much money could have a real, meaningful impact on people's health - but not if it's spent in the healthcare system. The further into this field I get, the more I realize how poor many of our diagnostic tests and therapeutic interventions are. Some are incredibly effective, but many of a middling efficacy, while a few other may not work at all. There are some interventions that we know work really well though - these are improved diet, increased exercise, quitting smoking, reducing stress, longer/improved sleep, and moderating alcohol consumption. The healthcare system is slowly beginning to focus on these highly important lifestyle factors, but because they're part of a person's lifestyle, they're affected by much more than just healthcare services.
The difference in healthcare spending between Canada and the US is about 6% of GDP. If Canada decided it could afford to spend an extra 6% of its GDP on improving health - roughly $100 billion each year - I'd much rather see it go to efforts to improve those metrics that we know work. Getting people to eat better or exercise more has always been a difficult challenge, but with $100 billion each year, I bet we could come up with a few things that'd have an impact.
This brings me to my main point - there's a reason to control costs in healthcare, because healthcare isn't the same as health and it's certainly not the same as life. We want good healthcare and I want to be part of providing it. But I want good healthcare because I want people (including myself!) to be happy and prosperous. If the costs of healthcare hinder those efforts by minimizing spending on other worthy pursuits more than they help directly by improving health, it's not really beneficial. There are diminishing returns when pumping more money into healthcare, especially when that additional money doesn't have a clearly established, useful purpose.
Bottom line - controlling health care costs, whether public costs paid through taxes or private costs paid through insurance premiums and out of pocket, is an important goal, even for those who want the healthiest people possible.
Match Day (well, not for me)
So, today was the CaRMS match day. Hundreds of graduating medical students just found out where they will spend the next 2-6+ years of their lives and what they'll be doing for the rest of their careers.
It's a day of very mixed emotions. For many, it's the best day of their lives. They get validation for 3-4+ years of hard work and learning. More importantly, they get a chance to help patients in the way they want to help patients, to have the career they wanted. Getting into medical school was a huge moment for me, but I'm not considering my career on track until I know my residency placement. I think a lot of students feel similarly, which is why getting a good result on Match Day is such a huge deal. It's a life-defining moment.
And yet, there are some who got less-than-stellar news today. There's always a percentage of people don't match each year in the first iteration. To them, it's a crushing moment, full of anxiety, fear, and uncertainty. Many will go through this whole process again with the unfilled spots left in the second iteration. By definition, these spots will be ones that had already rejected the unmatched applicants, or ones which those applicants chose not to apply to. That's a very tough pill to swallow - anything left that an applicant wants has basically already said "no", so they have to pursue programs they didn't want in the first place.
In the middle are people who matched, but went so far down their list of preferred programs that there's a major element of doubt. They'll be heading to a location or specialty they didn't fully expect to get, and have to make a major readjustment in mentality and life planning. That's a big curveball just when a career is starting to take off - and there's no backing out. CaRMS is a contract, so once you're matched, that's where you're going.
It's hard to know what to feel on days like today. Elation for some, cautious optimism for others, consolation for a few more.
Of course, being someone who will go through this all in a few short years, it's hard not to be a little scared of what's coming. Today's not about me - not even close - but it's tempting to put myself in the shoes of the current graduating class. To feel the unbridled excitement of matching to a first-choice program. To steel myself for the possibility that maybe I'll have to settle for a backup I never thought I'd end up with. To experience the dread of going unmatched and what I might do today to avoid that fate.
As I said - a day of mixed emotions.
It's a day of very mixed emotions. For many, it's the best day of their lives. They get validation for 3-4+ years of hard work and learning. More importantly, they get a chance to help patients in the way they want to help patients, to have the career they wanted. Getting into medical school was a huge moment for me, but I'm not considering my career on track until I know my residency placement. I think a lot of students feel similarly, which is why getting a good result on Match Day is such a huge deal. It's a life-defining moment.
And yet, there are some who got less-than-stellar news today. There's always a percentage of people don't match each year in the first iteration. To them, it's a crushing moment, full of anxiety, fear, and uncertainty. Many will go through this whole process again with the unfilled spots left in the second iteration. By definition, these spots will be ones that had already rejected the unmatched applicants, or ones which those applicants chose not to apply to. That's a very tough pill to swallow - anything left that an applicant wants has basically already said "no", so they have to pursue programs they didn't want in the first place.
In the middle are people who matched, but went so far down their list of preferred programs that there's a major element of doubt. They'll be heading to a location or specialty they didn't fully expect to get, and have to make a major readjustment in mentality and life planning. That's a big curveball just when a career is starting to take off - and there's no backing out. CaRMS is a contract, so once you're matched, that's where you're going.
It's hard to know what to feel on days like today. Elation for some, cautious optimism for others, consolation for a few more.
Of course, being someone who will go through this all in a few short years, it's hard not to be a little scared of what's coming. Today's not about me - not even close - but it's tempting to put myself in the shoes of the current graduating class. To feel the unbridled excitement of matching to a first-choice program. To steel myself for the possibility that maybe I'll have to settle for a backup I never thought I'd end up with. To experience the dread of going unmatched and what I might do today to avoid that fate.
As I said - a day of mixed emotions.
Sunday, 1 March 2015
Post-Conference Thoughts
Just returned from the conference, had a few thoughts.
1) Heated seats are possibly the best things in the world when you're driving for extended periods of time in the winter.
2) The conference was in Quebec and while it's been a while since I used it, I though my French was at least passable. It's not. Not even close.
3) A good portion of the conference was dedicated to a handful of topics and I found myself reminded of this comic:

1) Heated seats are possibly the best things in the world when you're driving for extended periods of time in the winter.
2) The conference was in Quebec and while it's been a while since I used it, I though my French was at least passable. It's not. Not even close.
3) A good portion of the conference was dedicated to a handful of topics and I found myself reminded of this comic:

(SMBC)
I don't mean to disparage the work of the conference attendees, most of whom had far more complex work to present than I did and generally presented it better as well, but there did seem to be a lot of energy devoted to one or two topics in medicine with little attention paid to other meaningful research pursuits.
Part of this is the nature of the conference of course, no conference is universal in scope even when restricted to certain disciplines, but it's true for research in general as well. Some topics seem to get an inordinate amount of attention and funding, even for relatively trivial aspects of that subject, while other fields are almost devoid of attention.
This would be reasonable if those areas of research with intense activity answered the key questions reliably, but that doesn't necessarily happen. There are a lot of low-quality studies out there, ones that address the question, but come with so many asterisks that the conclusions are not necessarily reliable. Such studies can be useful when first addressing a problem - they can provide descriptive information, generate hypotheses, and identify research areas clearly not worth pursuing. Yet, once a field has been established, these studies can only pick at the margins, rather than provide any real clarity.
For all the time, energy, and resources put into the research presented at the conference, one good RCT or high-quality cohort study would likely have been more meaningful. That would require concentrating resources, however, while the current model for research funding tends to spread out resources between groups. That means a lot of researchers producing necessarily flawed studies because none of them can afford to do a high-quality one.
In a lot of activities, I've found you get credit either for doing something exceptionally well, or doing something exceptionally unique. Research appears to be much the same. I do hope to get to do that high-quality, question-answering research in the future, when I have a bit more clout than I do as a pre-clerkship MD candidate. For now, doing relatively unique research has been quite interesting and, I hope, useful.
P.S. Oh yeah, this. An exaggeration? Yes. A huge exaggeration? Nope...

P.S. Oh yeah, this. An exaggeration? Yes. A huge exaggeration? Nope...
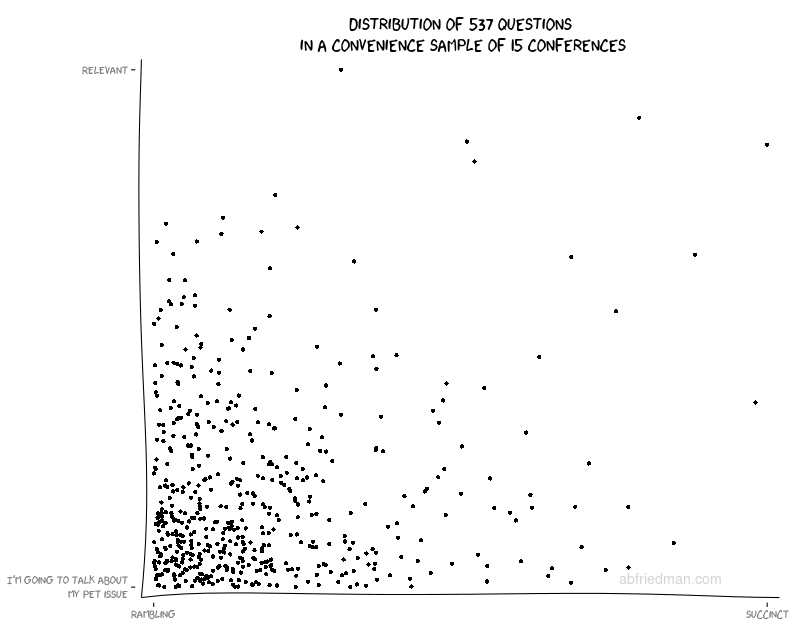
(Ari Friedman via The Incidental Economist)
Subscribe to:
Posts (Atom)